1/ Another THREAD on nerve entrapment...
This time the victim is the TIBIAL NERVE (TN).
“Tibia” is Latin for “shinbone” AND “flute”... but what about a “flute” made of “shinbone”??
Yep, that happened. Here’s a copy of a Tibial Flute originally made 10,000 yrs ago in Germany...
This time the victim is the TIBIAL NERVE (TN).
“Tibia” is Latin for “shinbone” AND “flute”... but what about a “flute” made of “shinbone”??
Yep, that happened. Here’s a copy of a Tibial Flute originally made 10,000 yrs ago in Germany...

2/ Time for a little anatomy review.
The TN splits off the sciatic nerve and is sometimes called the “Posterior Tibial Nerve” in the lower leg.
The TN splits off the sciatic nerve and is sometimes called the “Posterior Tibial Nerve” in the lower leg.
3/ The TN is commonly vulnerable to entrapment at 2 sites:
1) Tibial Tunnel (TT)
2) Proximal Soleus (SSS... explained later)
Let’s dive into 1)...
1) Tibial Tunnel (TT)
2) Proximal Soleus (SSS... explained later)
Let’s dive into 1)...
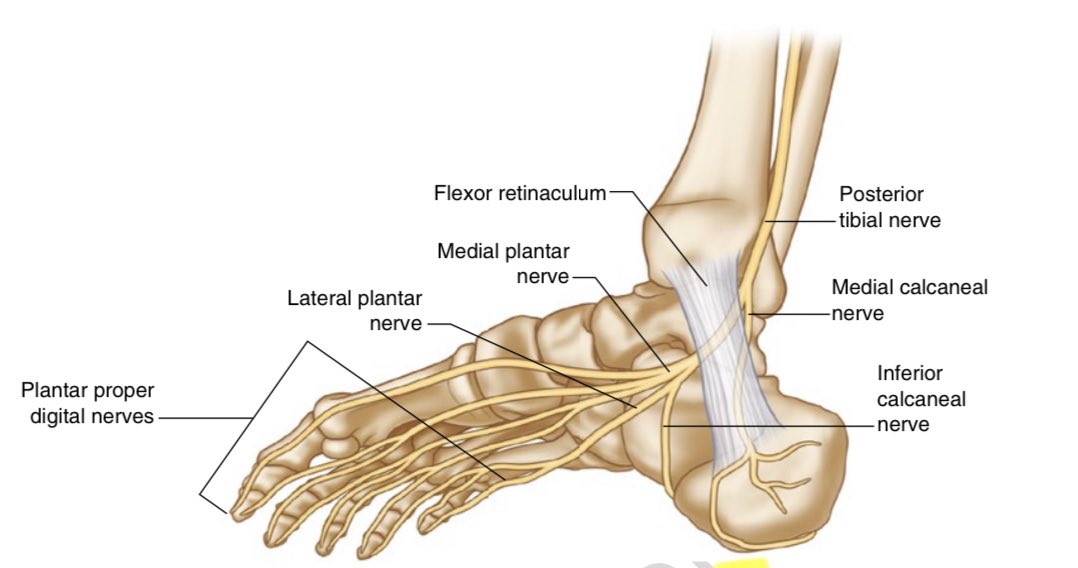
4/ The TT travels along the posterior-medial ankle,
has the flexor retinaculum as its ceiling and
its bony floor consists of the posteromedial talus, the medial navicular, & the medial calcaneus.
has the flexor retinaculum as its ceiling and
its bony floor consists of the posteromedial talus, the medial navicular, & the medial calcaneus.

5/ It contains (from anterior to posterior):
“TOM” - the tibialis posterior (TP) tendon,
“DICK” - the flexor digitorum longus (FDL) tendon,
“&” - the TN neurovascular bundle,
“HARRY” - the flexor hallucis longus (FHL) tendon.
“TOM” - the tibialis posterior (TP) tendon,
“DICK” - the flexor digitorum longus (FDL) tendon,
“&” - the TN neurovascular bundle,
“HARRY” - the flexor hallucis longus (FHL) tendon.

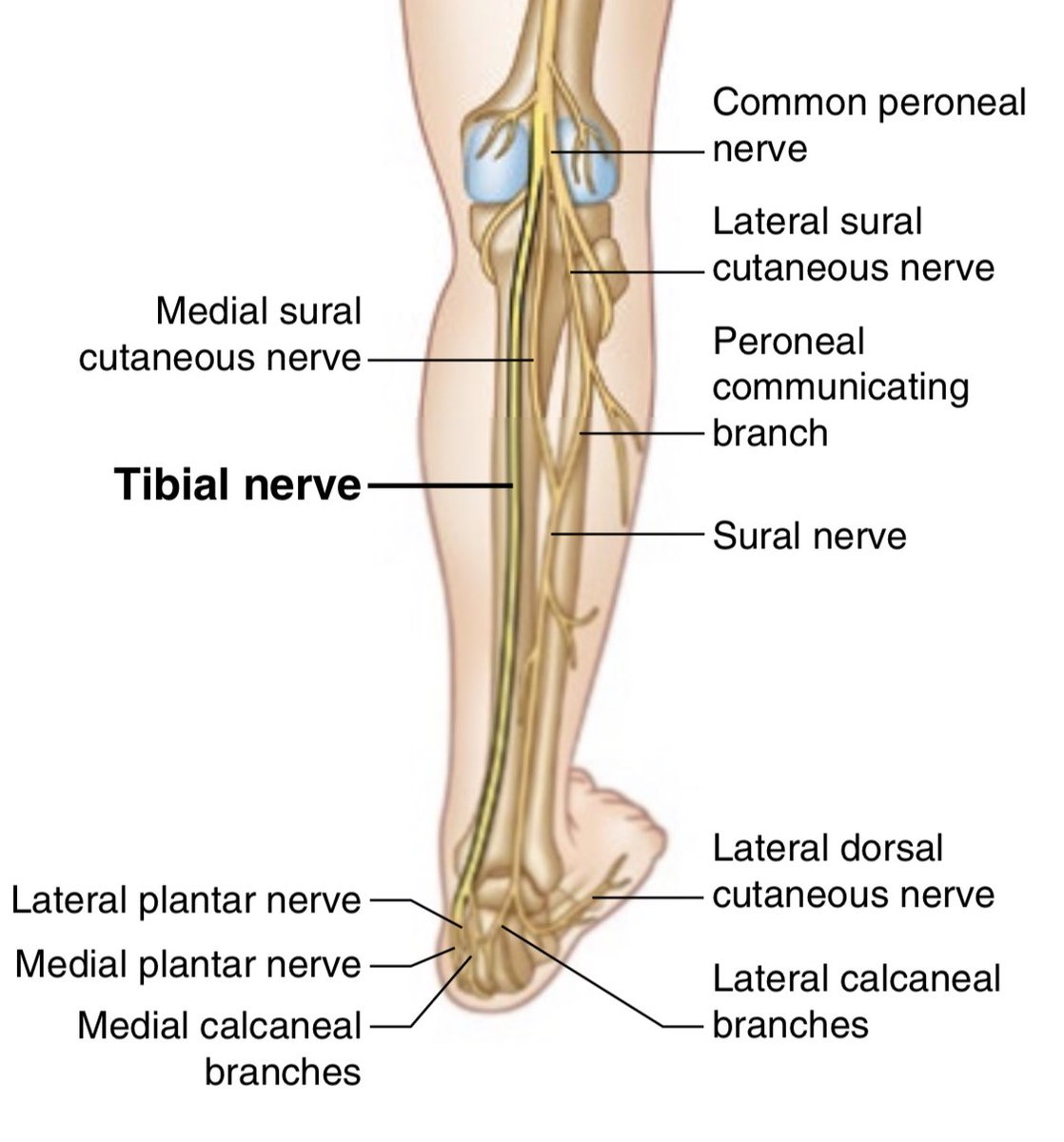
6/ The TN gives off the medial calcaneal nerve (MCN) just prior to entering the tunnel,
and splits within/soon after exiting the tunnel to form the lateral plantar nerve (LPN), medial plantar nerve (MPN), & Inferior Calcaneal Nerve (ICN).
👉* Remember ICN & MPN *👈
and splits within/soon after exiting the tunnel to form the lateral plantar nerve (LPN), medial plantar nerve (MPN), & Inferior Calcaneal Nerve (ICN).
👉* Remember ICN & MPN *👈
7/ Methods of entrapment:
• ankle DF & Eversion
• history of foot/ankle fracture/dislocation
• pronated foot
• edematous conditions
These conditions could create a tension entrapment at the distal end of the tunnel.
• ankle DF & Eversion
• history of foot/ankle fracture/dislocation
• pronated foot
• edematous conditions
These conditions could create a tension entrapment at the distal end of the tunnel.
8/ What you *could* find in the clinic w/ TT Entrapment:
• local and radiating symptoms with palpation of the tunnel
• weak flexion of toes
• weak big toe aBDuction (secondary effect)
• sensory changes along sole of foot (burning pain, tingling, numbness)
• local and radiating symptoms with palpation of the tunnel
• weak flexion of toes
• weak big toe aBDuction (secondary effect)
• sensory changes along sole of foot (burning pain, tingling, numbness)
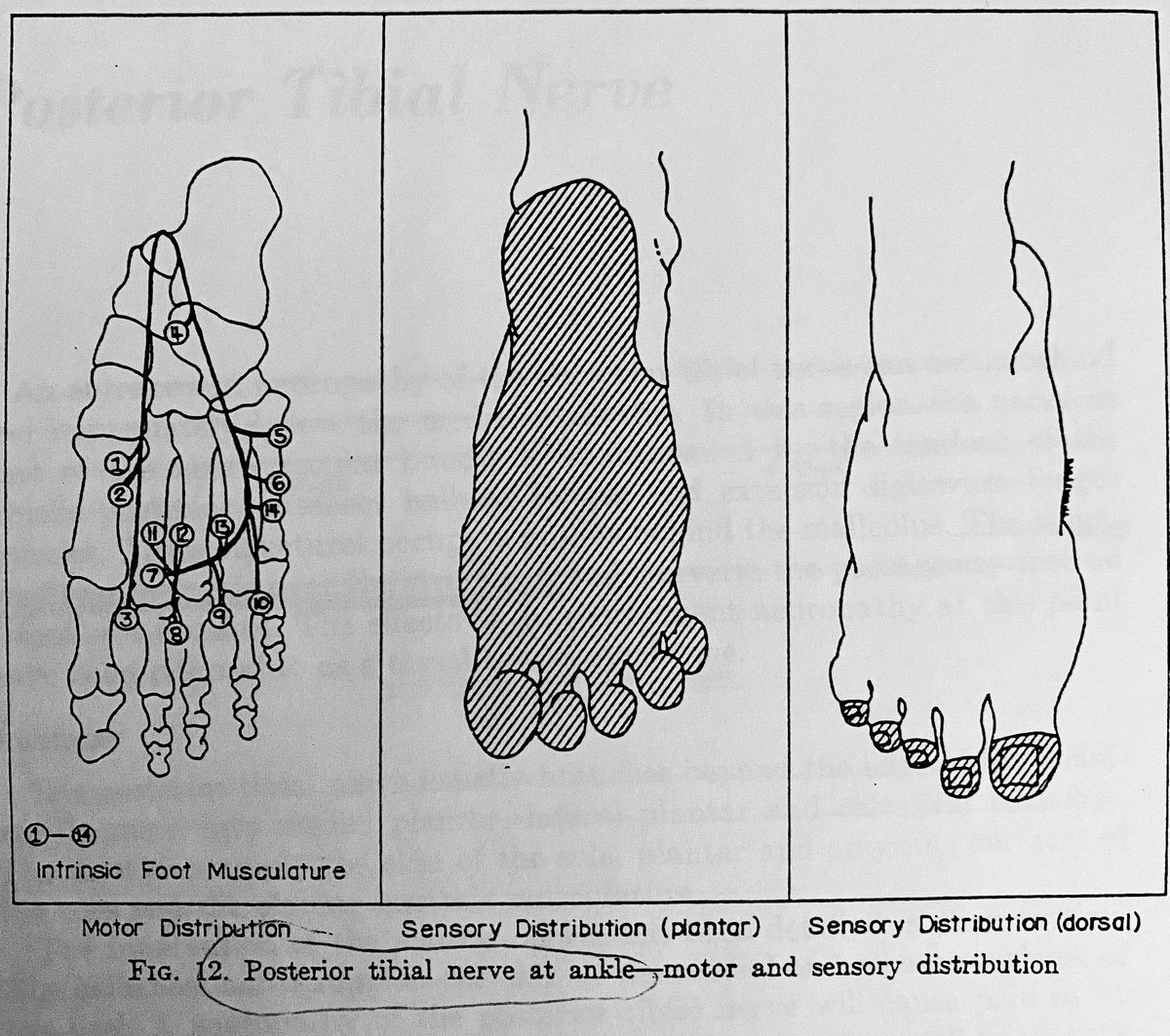
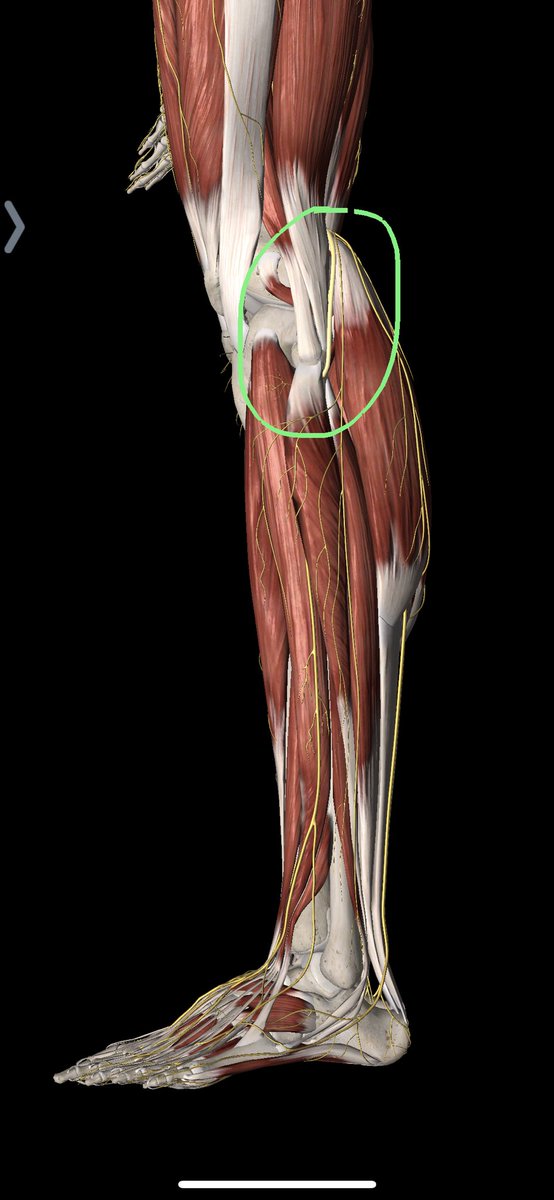
9/ So, why point out the MPN & ICN earlier?
Think back to people with sharp pain in the yellow circle marked below.
Yeah...
That’s right... “PLANTAR FASCIITIS” could be neurogenic!!!
Think back to people with sharp pain in the yellow circle marked below.
Yeah...
That’s right... “PLANTAR FASCIITIS” could be neurogenic!!!

10/ In some cases of “plantar fasciitis” folks end up “failing” conservative treatments because nobody took the time to check for neurogenic causes of their pains!
11/ Let’s move on to a less common TN entrapment site...
Entrapment at Proximal Soleus (called the Soleus Sling Syndrome) occurs where it passes through a tunnel between the superficial and deep posterior compartments of the leg at the origin of the soleus muscle.
Entrapment at Proximal Soleus (called the Soleus Sling Syndrome) occurs where it passes through a tunnel between the superficial and deep posterior compartments of the leg at the origin of the soleus muscle.
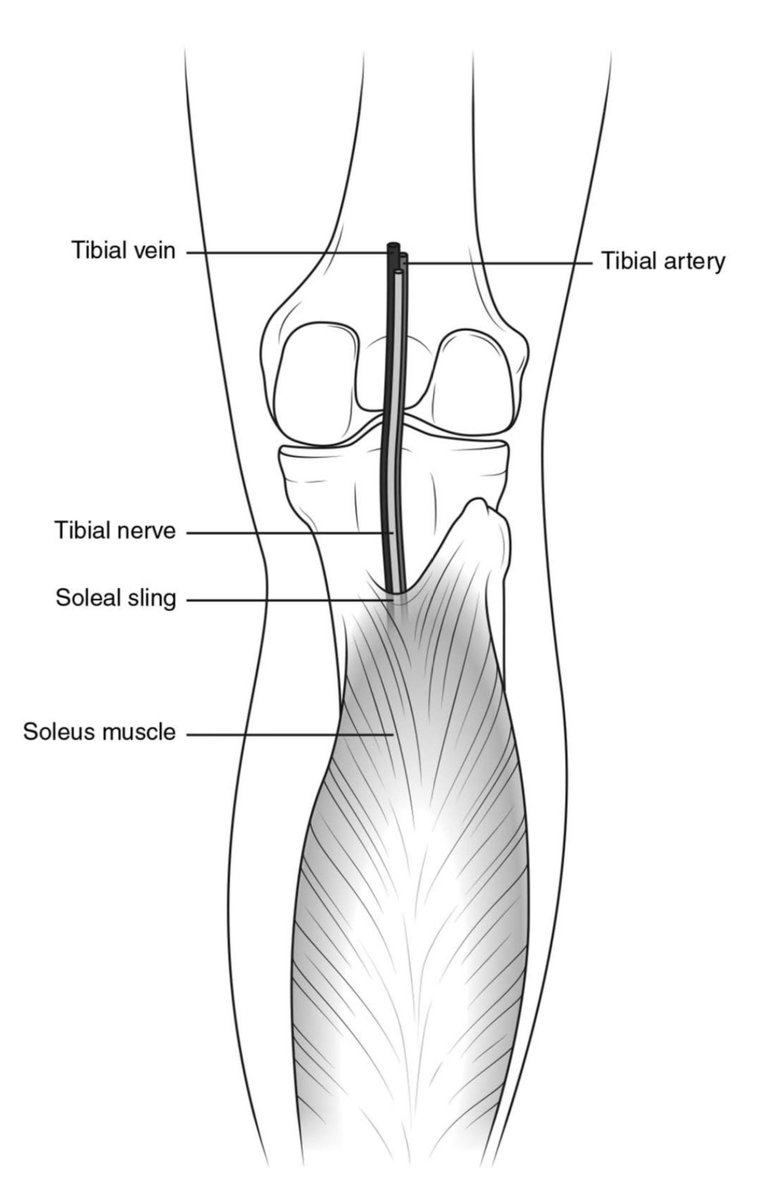
12/ SSS presents with:
• pain in the popliteal fossa and proximal calf (aggravated by active and passive dorsiflexion of the foot)
• inability to bear weight
• weakness of toe flexion
• sensory deficits on the sole of the foot
All of which are aggravated by walking.
• pain in the popliteal fossa and proximal calf (aggravated by active and passive dorsiflexion of the foot)
• inability to bear weight
• weakness of toe flexion
• sensory deficits on the sole of the foot
All of which are aggravated by walking.
13/ Clinical note:
People reporting of persistent posterior leg “tightness” should be checked for neurogenic involvement.
For these folks, stretching doesn’t help, but they can’t stop stretching their hamstrings/calves!
Think: repetitive hamstring tears, calf strains, etc.
People reporting of persistent posterior leg “tightness” should be checked for neurogenic involvement.
For these folks, stretching doesn’t help, but they can’t stop stretching their hamstrings/calves!
Think: repetitive hamstring tears, calf strains, etc.
14/ Common conservative treatment strategies?
• orthotics
• address pathomechanics involved with foot pronation & excessive hind foot eversion
• check shoes
• check running form & walking mechanics
• check hip mobility
• orthotics
• address pathomechanics involved with foot pronation & excessive hind foot eversion
• check shoes
• check running form & walking mechanics
• check hip mobility
15/ IF full trials of conservative strategies fail, then neurolysis may be indicated.
Better evaluation begets better treatment strategies.
Like a mentor of mine once said:
“If you aren’t looking for it, then you won’t see it.”
Better evaluation begets better treatment strategies.
Like a mentor of mine once said:
“If you aren’t looking for it, then you won’t see it.”
Extra: apparently bone flutes can still be purchased in Europe...
trinoxsamoni-lutherie.com/products/bone-…
trinoxsamoni-lutherie.com/products/bone-…
• • •
Missing some Tweet in this thread? You can try to
force a refresh