Data Update: Suicide Subpopulations in 2020
Colorado Subgroup Data is out, so I can focus on demographic groups in a major US State. Colorado has ~5.8 million people.
Let's look overall at the state first. The suicide rate decreased* in 2020 by a small amount (2.3%).
/1
Colorado Subgroup Data is out, so I can focus on demographic groups in a major US State. Colorado has ~5.8 million people.
Let's look overall at the state first. The suicide rate decreased* in 2020 by a small amount (2.3%).
/1

It should be noted that this rate of suicide is quite high. Colorado ranks 6th among states for suicide.
Let's break it down by gender:
In Colorado, suicide rates for men were essentially unchanged, and there was a minor decrease* in the rates for women.
/2
Let's break it down by gender:
In Colorado, suicide rates for men were essentially unchanged, and there was a minor decrease* in the rates for women.
/2

By CDC Race categories*:
We see it was only white Coloradans that overall had a suicide rate decrease*. All non-white Coloradans displayed an increased* rate in 2020 by varying degrees. Indigenous suicides by # are smaller and show variance but by rate dwarf the others.
/3
We see it was only white Coloradans that overall had a suicide rate decrease*. All non-white Coloradans displayed an increased* rate in 2020 by varying degrees. Indigenous suicides by # are smaller and show variance but by rate dwarf the others.
/3

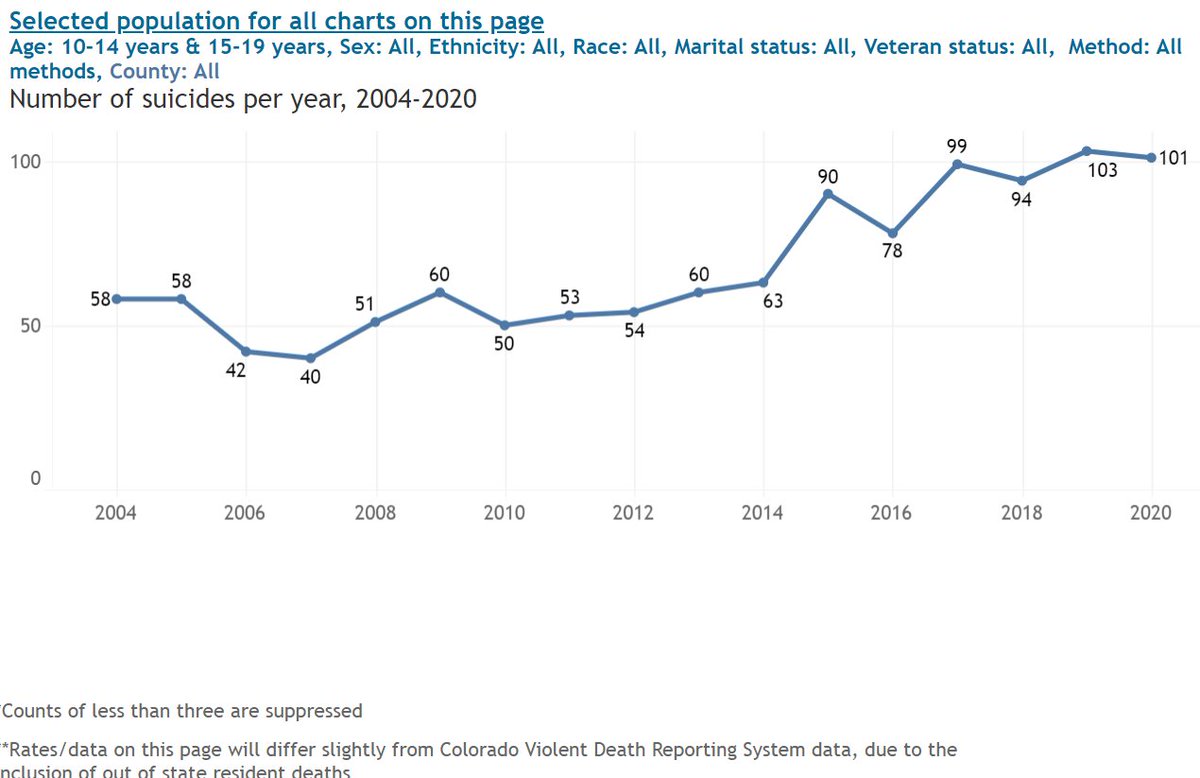
Here we have the long-awaited youth data!
There was no significant change in suicide rates for Coloradans under 20.
For youth subgroups:
White youth: slight increase*
Nonwhite youth: slight decrease*
Male: slight decrease*
Female: no change*
/4
There was no significant change in suicide rates for Coloradans under 20.
For youth subgroups:
White youth: slight increase*
Nonwhite youth: slight decrease*
Male: slight decrease*
Female: no change*
/4
* Note that for all comparisons from 2019-2020, NONE (increase are decrease) are outside of the expected variance based upon comparing two proportions. However as this is the whole state population, increases and decreases are characterizable.
/5
/5
Suicides by gun were unchanged.
/6
/6

• • •
Missing some Tweet in this thread? You can try to
force a refresh