
For those of you interested in multiple myeloma, here is a brief state of the science for treatment.
1/ For newly diagnosed patients, triplets, VRd or DRd, are the standard of care. Current RCTs are examining if we can improve outcome using quadruplets. Eg. PERSEUS trial.
1/ For newly diagnosed patients, triplets, VRd or DRd, are the standard of care. Current RCTs are examining if we can improve outcome using quadruplets. Eg. PERSEUS trial.

2/ In newly diagnosed myeloma, another question given the cost & potential toxicity of quadruplets is to start with a triplet, and based on MRD status identify patients who need 4 drugs versus this who do equally well with 3 drugs. Eg: EQUATE trial. @myelomaMD @mtmdphd @eaonc
3/ Auto stem cell transplant is still standard of care for eligible patients. Current data indicate overall survival is similar whether the transplant is done early or delayed. But for many reasons we prefer early transplant for most patients.

4/ Lenalidomide maintenance is standard of care after initial therapy. For high risk patients, lenalidomide + bortezomib. Current research questions include whether we can stop maintenance after 2 years, or adjust maintenance based on MRD status. Eg: SWOG trial; OPTIMUM trial


5/ For Relapsed myeloma numerous treatments are being investigated alone and in combination across the world. The more active drug classes we have, the longer the survival. Great progress.

6/ Immunotherapy is the major advance in myeloma. Bispecific antibodies and CAR-T cell therapy hold great promise. Multiple options available for myeloma refractory to lenalidomide, pomalidomide, bortezomib, carfilzomib, daratumumab, isatuximab, alkylators, and transplant.

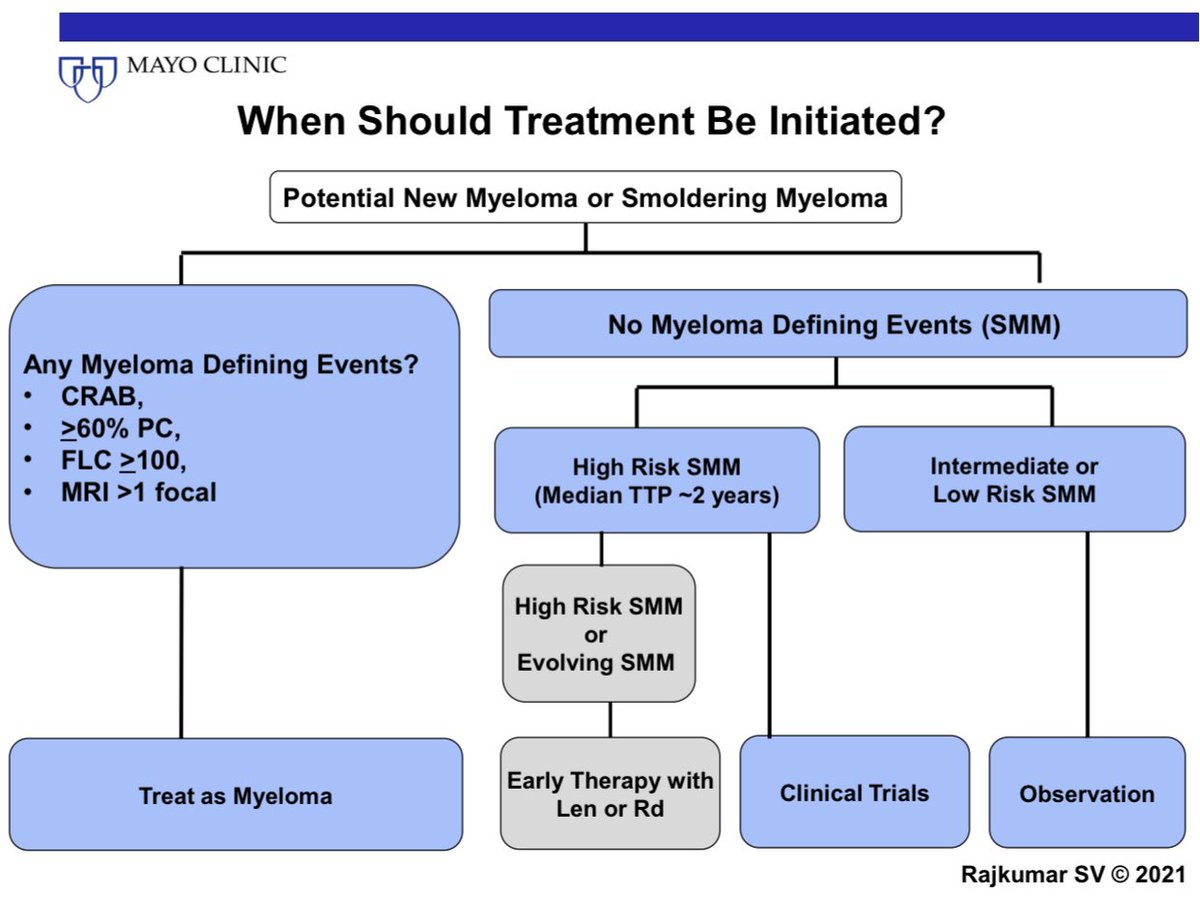
7/ For smoldering myeloma, we now feel that early therapy is indicated for high risk patients. A comprehensive trial strategy is underway, specifically to see if patients with high risk SMM do better with myeloma like treatment like DRd, or if mild treatment like Rd is enough.

• • •
Missing some Tweet in this thread? You can try to
force a refresh


















