
ACIP's slides on mRNA vaccines and myocarditis are now available cdc.gov/vaccines/acip/…
Hard to argue this isn't causal
Hard to argue this isn't causal

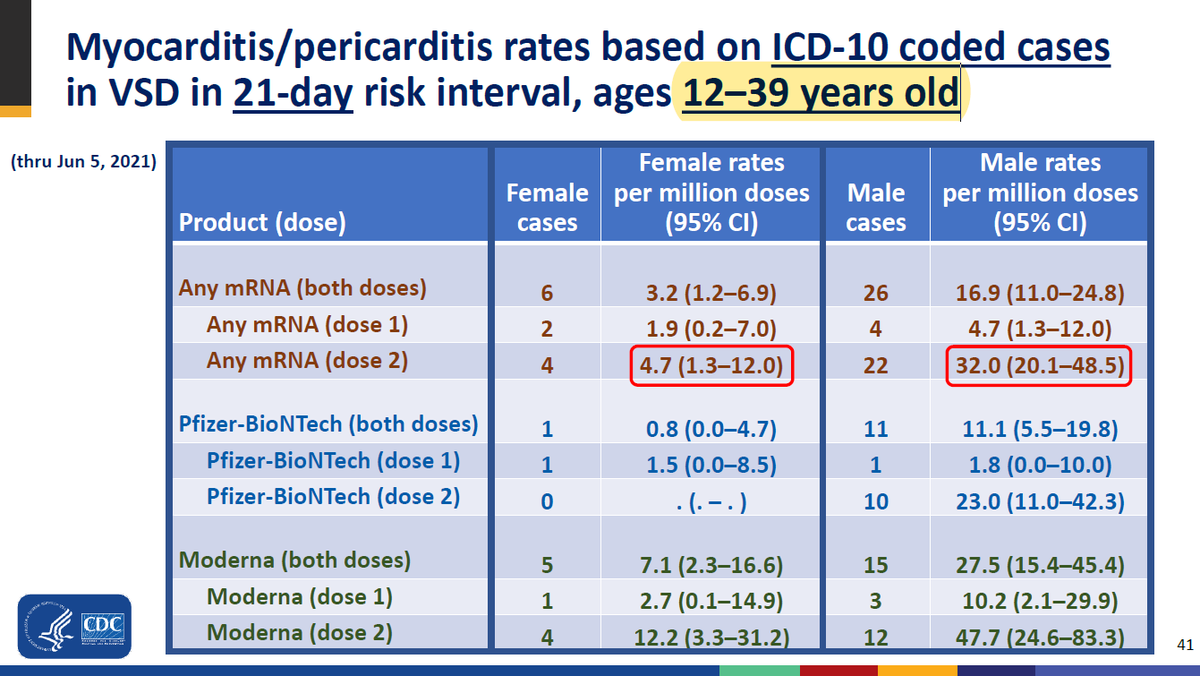
The signal by age and dose is not ambiguous

Risk clearly seems highest among young males

Important to note: anyone can report anything to VAERS
When they dig into 29 *confirmed* cases:
- majority were hospitalized
- 2 required ICU care
- all were eventually discharged
When they dig into 29 *confirmed* cases:
- majority were hospitalized
- 2 required ICU care
- all were eventually discharged

The rates here are a bit misleading because teens are lumped in with twenty- and thirtysomethings. (To be fair, they have to do this because counts are so low.)
It's fair to call vaccine-associated myocarditis rare or very rare. And it's reassuring that most of those who develop it do well.
Still waiting to see more detail from Israel sciencemag.org/news/2021/06/i…
Still waiting to see more detail from Israel sciencemag.org/news/2021/06/i…

I am a big proponent of vaccination, but I think it's fair to ask a question:
What is the incremental benefit of a second dose in young males (say, under 25), especially as more and more older people are fully vaccinated?
/ end
What is the incremental benefit of a second dose in young males (say, under 25), especially as more and more older people are fully vaccinated?
/ end
• • •
Missing some Tweet in this thread? You can try to
force a refresh











