
Had a blast returning to in-person morning report at @VAPaloAlto! Some learning points: [1/5] 

1. Strep intermedius can be normal oral flora, but can be very immunogenic and tends to form abscesses. See this excellent review in Frontiers! frontiersin.org/articles/10.33…
[2/5]
[2/5]
2. When managing an empyema (or complicated pleural effusion), involve your thoracic surgical colleagues early as aggressive source control is paramount. [3/5]
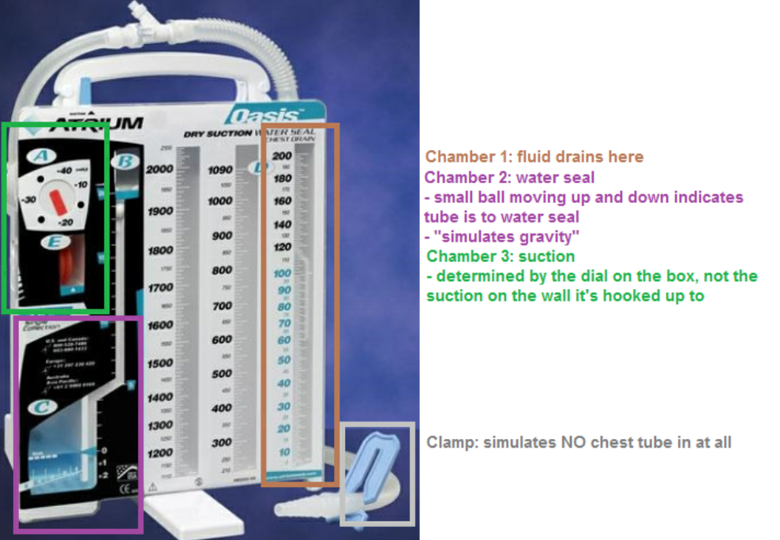
3. What do all those chest tube settings mean?
-clamped: simulates no chest tube
-water seal: 'passive' drainage of the fluid/air out
-suction: low-level continuous negative pressure to help draw the fluid/air out [4/5]
-clamped: simulates no chest tube
-water seal: 'passive' drainage of the fluid/air out
-suction: low-level continuous negative pressure to help draw the fluid/air out [4/5]
4. Why use 'water seal' anyway? If you only had one container to pull out fluid, it would only pull until pressures were equal. And fluid could go back in the pleural space when the patient inhales! (credit to former chief Andre Kumar for first teaching us this schematic!) [5/5]

• • •
Missing some Tweet in this thread? You can try to
force a refresh





