
1/ #IDTwitter #HIVTwitter #HIVDrugResistance
To keep the momentum going, let’s move on to transmitted drug resistance. For those just joining, we previously discussed that #HIVDrugResistance is important yet challenging for learners.
To keep the momentum going, let’s move on to transmitted drug resistance. For those just joining, we previously discussed that #HIVDrugResistance is important yet challenging for learners.

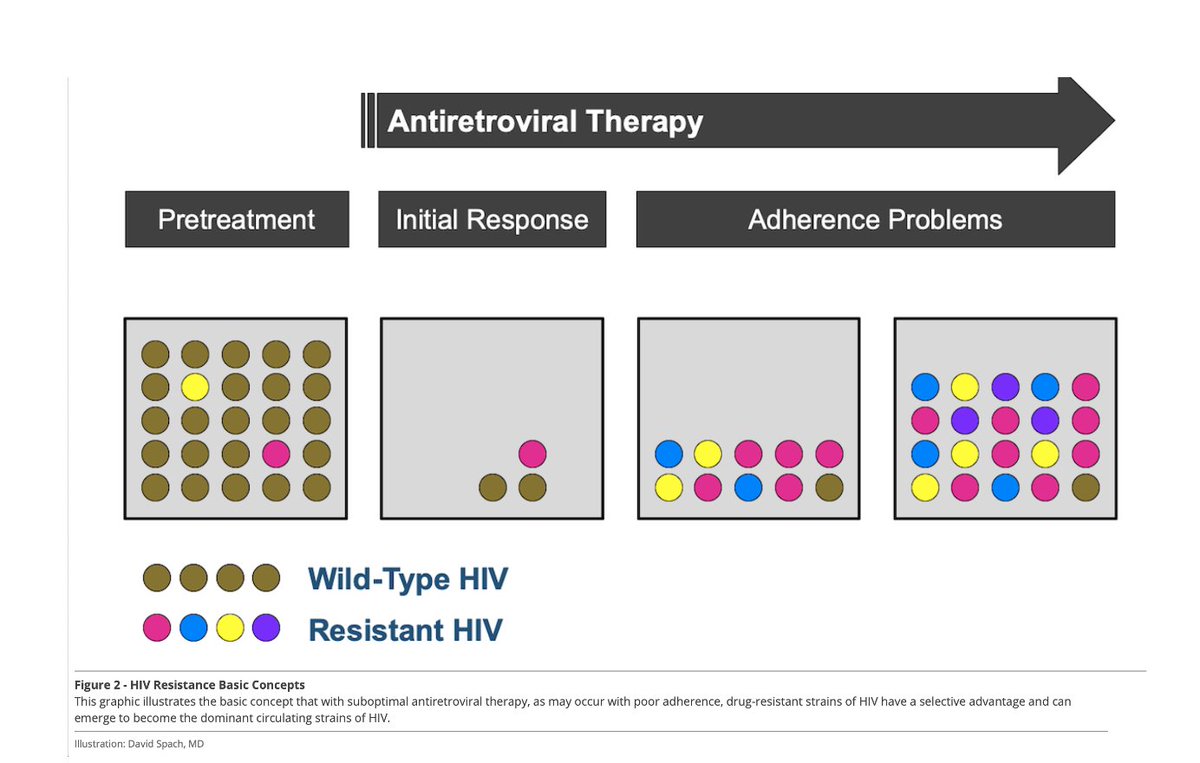
2/ We also reviewed the basic principle that HIV resistance develops when HIV replicates in the setting of subtherapeutic drug levels. Virions containing resistance mutations are selected for in this case.

3/ Today we’ll define transmitted drug resistance (TDR) (vs acquired drug resistance). TDR = acquisition of drug-resistant HIV at the time of new HIV infection. We identify TDR when we do a baseline HIV genotype (recommended for all patients who are newly diagnosed with HIV).
4/ Interestingly, as @PaulSaxMD points out, a baseline HIV genotype (to detect TDR) is a nice to know but not a need to know piece of info. With same day ART starts, we start patients on therapy before we know the results of their HIV genotype.

5/ We can get away with this because we use INSTI-containing regimens for all of our 1st line therapy. Rates of TDR impacting our 1st line therapies are exceedingly uncommon. (1st line recommended regimens in the US summarized by @febrilepodcast below).

6/ Lucky for me, a nice updated on TDR just came out in CID. Rates of TDR in the US between 2014-2018 are shown below. doi.org/10.1093/cid/ci…

7/ The most common mutation detected was the K103N (8.6%). M184V (0.9%) & K65R (0.1%), less common. We will discuss these mores when we get into specific mutations. Should clarify this data is specific to US; global TDR beyond scope here.
8/ Transmitted drug resistance is very difficult if not impossible to predict. Acquired drug resistance, on the other hand, develops while someone is on therapy. This can occur when someone receives an inadequate regimen and/or is nonadherent to their therapy.
9/ Next time we will discuss when and how to test for acquired drug resistance. For now, remember the #keyclinicalcorrelate that all patients should receive a baseline HIV genotype upon diagnosis to check for transmitted drug resistance.

10/ With the caveat that results of a baseline HIV genotype do not necessarily change what regimen we will start. Additionally, current guidelines do not recommend obtaining resistance testing to INSTIs. This makes sense given the low rates of INSTI TDR.

11/ But as INSTIs are used with increased frequency, this may change. For now though, only genotypic resistance to evaluate for NRTI, NNRTI, and PI resistance is recommended. clinicalinfo.hiv.gov/en/guidelines/…
12/ Stay tuned for our next episode when we will review the different types of #HIVDrugResistance tests and how they are done.

• • •
Missing some Tweet in this thread? You can try to
force a refresh






