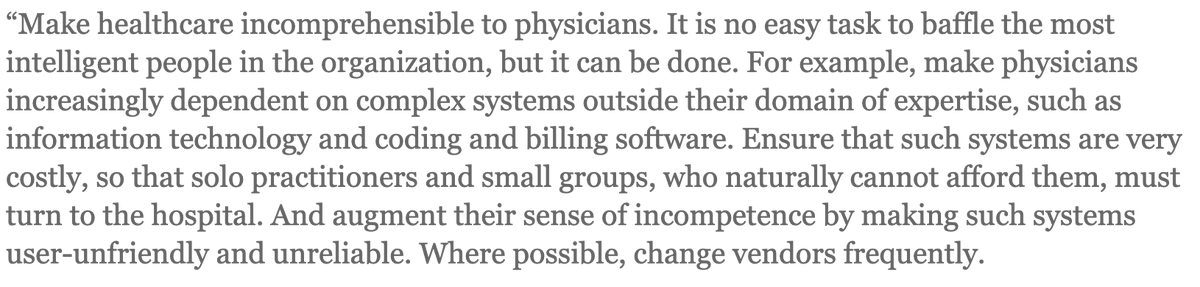
Every physician, fellow, resident and medical student should read this article. It remains as relevant as the time it was written in 2014. I will share excerpts that I believe most exemplify what we are experiencing today. They thehealthcareblog.com/blog/2014/09/1…
2)clarify the tactics used by corporate entities to control physicians who are strong patient advocates. And my suggestions on ways to take our power back. Unfortunately, the vitriol that docs think we are gods is prevalent. The toxic environment in which docs are trained
3)today virtually ensures that is not the case. Nevertheless, the false claim still prevails. Doesn't help to have virtue-signaling docs perpetuate the hype. Docs, you matter and patients matter. Never forget that, despite the gaslighting. 

4)One good answer to this intent to "baffle". Direct Primary Care(DPC). Self-employed docs control their own destiny. Quality(not quantity) of care trumps everything. The patient-doctor relationship is just as important to patients as it is to docs. No meddling middlemen.
5)Confidence is maintained in knowing that you know medicine-they don't. Also, never keep all your eggs in one basket. Termination is a risk when one cannot be controlled. Keep yourself marketable)clean record, excellent LORs, etc.). No favors. Company needs my services-pay me.

6)I reiterate, you know medicine, they don't. Don't allow businesspeople to convince you otherwise. You know exactly how you were trained. Remember your oath.

7)This is why I do not subscribe to the term "Provider". Medicine is a not a fast food joint and patients are not customers/clients. These business terms are dehumanizing(as they are meant to be). I cater to patients, not metrics. For that reason, always have two jobs.

8)Again, f**k metrics and patient satisfaction scores. Put the patient first and keep them there. Want your quality to suffer, then let metrics be your guide. And your liability will increase. Anybody can sue, but not everyone wins. Take care of your patients right, they win, you

9)win. Again, always have two jobs. This last "strategy" I find to be the most despicable. It is why patients can now go to a hospital and only be seen by NPPs from admission to D/C, no physician in sight. This is where corporate medicine has won. The patients and/or their

10)families have the right to request a physician. FYI, every department has a medical director. They are physicians and fully capable of seeing patients. Anyone permitting this kind of irresponsible practice in their department is accountable, as is the facility. Chronic
11)understaffing of physicians is a choice and a business decision that doesn't have anything to do with patient care. @pppforpatients @PPA_USA @TakeMedBack
• • •
Missing some Tweet in this thread? You can try to
force a refresh