
1/ #IDTwitter #HIVTwitter
Today we will review some of the common types of #HIVDrugResistance tests.
Today we will review some of the common types of #HIVDrugResistance tests.

2/ I first break down testing into 2 broad categories of resistance tests:


4/ In a standard genotype test, a patient’s circulating HIV is isolated, amplified by PCR, and reverse transcribed in vitro to DNA. The polymerase (RT), protease, and integrase genes can then be sequenced and compared to wildtype (more on this in 10-12).

5/ #KeyClinicalCorrelates for standard genotypes:
-pts have to be viremic (doesn’t work for patients who are suppressed)
-not all standard genotypes include integrase (may need order separately)
-only mutations present in ~80% are typically detected.
-pts have to be viremic (doesn’t work for patients who are suppressed)
-not all standard genotypes include integrase (may need order separately)
-only mutations present in ~80% are typically detected.
6/ In archived genotypes, cell-associated proviral HIV DNA is isolated from whole blood, amplified, sequenced, and compared to wildtype (more on this in 10-12).

7/ Studies are mixed on how well standard and archived genotypes correlate. Standard HIV genotypes are still the preferred tests. Archived genotypes are specific but sometimes lack sensitivity.
8/ If you see a resistance mutation in an archived geno, you can be sure it’s real. If you don’t see a mutation you are expecting based on pt hx, you might want to work under the assumption that it’s there even if not detected by the archived geno.
9/ The major advantage of an archived genotype is that you can do it when a patient is suppressed.
10/ Whether you do a standard or an archived genotype, you will get a sequence that can be compared to wildtype sequence. Recall that the DNA sequence predicts an RNA sequence which predicts an amino acid sequence.
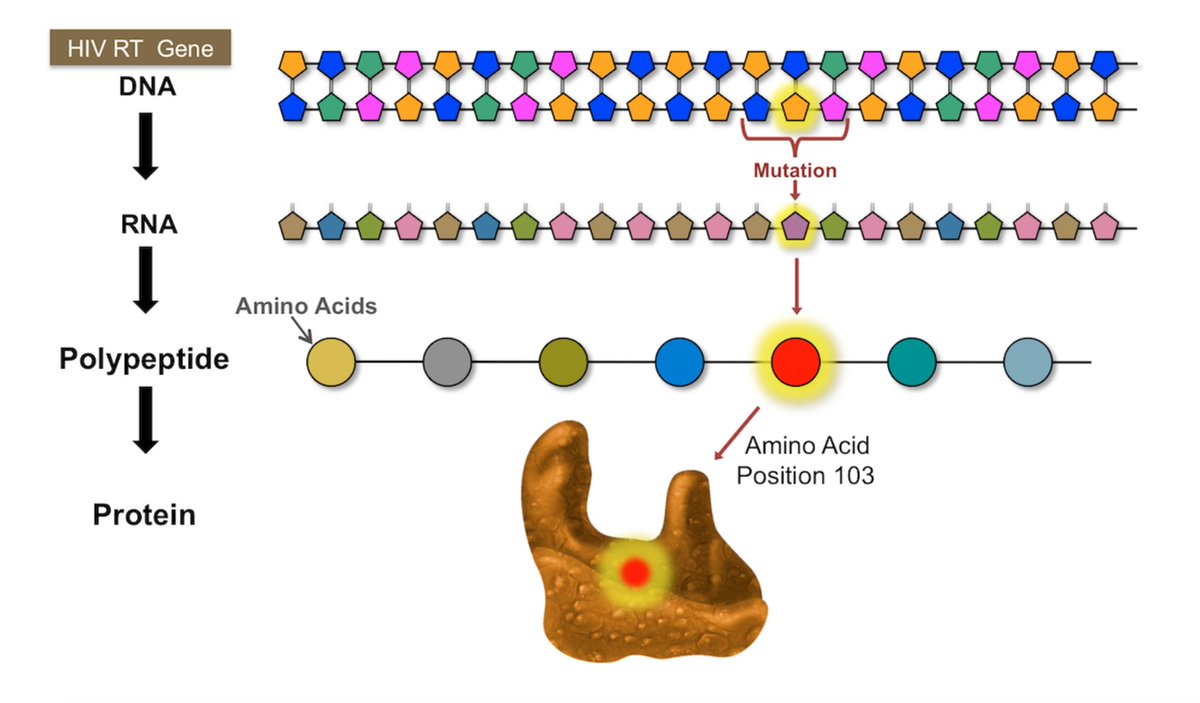
11/ There are well-defined amino acid substitutions that we know, when present, will render specific ARVs resistant. Ex: A mutation that leads to a substitution of lysine (K) for asparagine (N) at position 103 in the RT gene results in resistance to nevirapine and efavirenz.

12/ This graphic emphasizes the nomenclature we use for describing genotype resistance mutations.

13/ Let's move on to phenotypes.
HIV phenotype testing is not done as often as genotype testing because it is expensive and time-consuming. The concept of this test is analogous to determining MICs in vitro for antibiotics against bacterial pathogens.
HIV phenotype testing is not done as often as genotype testing because it is expensive and time-consuming. The concept of this test is analogous to determining MICs in vitro for antibiotics against bacterial pathogens.
14/ In phenotype testing, virus from a patient is isolated and the viral genes (RT, protease) are amplified and then inserted into a lab strain of HIV without these genes. These recombinant clones are then tested for drug susceptibility in vitro.
15/ The phenotype test measures and reports the IC50 or the drug concentration required to inhibit replication of the patient’s HIV by 50%. This is then compared to wildtype strains. The further the patient’s curve is shifted to the right, the higher degree of resistance.

16/ We will talk about indications for resistance testing and when you might choose on over another next time.

17/ For now, remember that like any test, an #HIVDrugResistance test can never be interpreted in isolation. A patient’s ART history, adherence history, and prior resistance tests are all essential in helping interpret resistance tests and making management decisions.
• • •
Missing some Tweet in this thread? You can try to
force a refresh





