80% [78,82] of England's Total population have now been vaccinated or infected
Wall of immunity:
10% Infected only
19% Both infxn+vax
51% Vaccinated 1or2 doses
Usual caveats: time lag after vax, not 100% protective, assumes random vaxing probability of previously infected etc
Wall of immunity:
10% Infected only
19% Both infxn+vax
51% Vaccinated 1or2 doses
Usual caveats: time lag after vax, not 100% protective, assumes random vaxing probability of previously infected etc

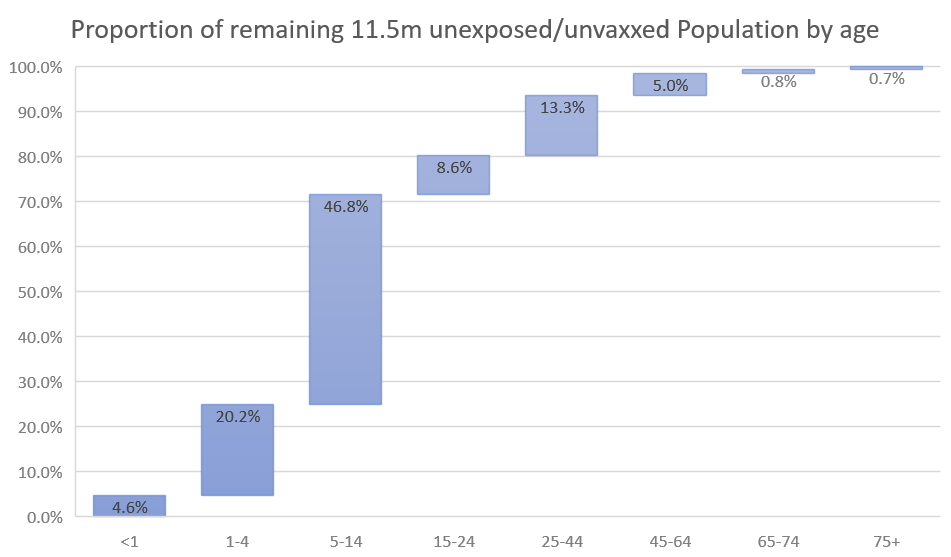
Remaining 11.5m unexposed/unvaxxed susceptible population is heavily skewed to younger age groups.
80% under 25yo
47% in school age kids 5-14yo
Outbreaks and cases will expectedly be concentrated in these groups now and increasingly <15 after current vax roll out plan completed
80% under 25yo
47% in school age kids 5-14yo
Outbreaks and cases will expectedly be concentrated in these groups now and increasingly <15 after current vax roll out plan completed
Quick check of the model against ONS serosurvey and PHE blood donor antibody surveillance, in 16yo+:
Model 95.8% (up to 8 August)
ONS 93.6% (12 - 19 July)
PHE 96.2% (28 June - 23 July)
Looks okay.
Model 95.8% (up to 8 August)
ONS 93.6% (12 - 19 July)
PHE 96.2% (28 June - 23 July)
Looks okay.

Expecting blood donors to be slightly more likely to be vaxxed (engaging with health services) and higher exposure/socially engaged.
3 weeks since ONS Ab data more than made up for by additional infections and vaxxing.
3 weeks since ONS Ab data more than made up for by additional infections and vaxxing.
Overall the wall looks solid.
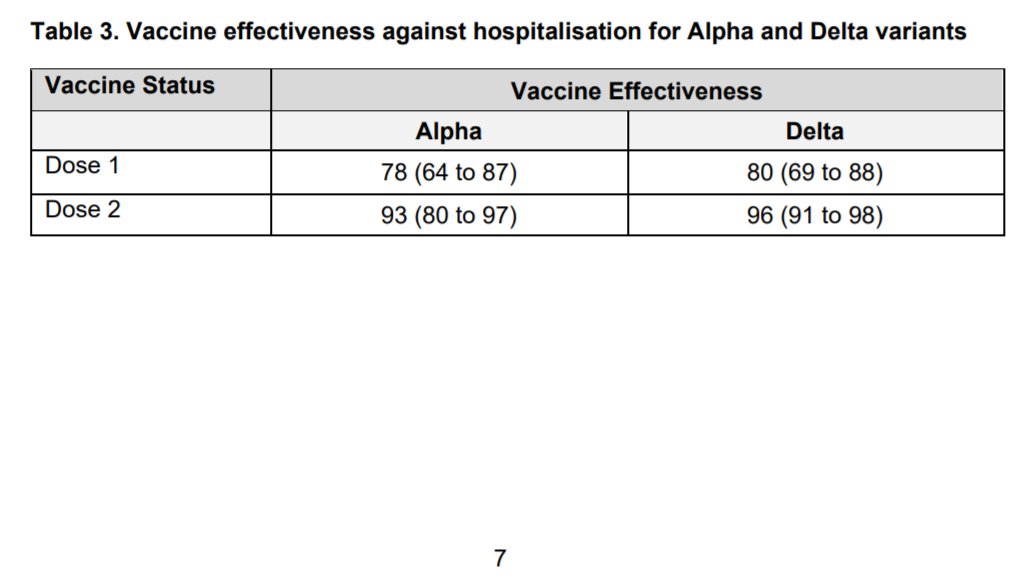
PHE analysis suggests 96% vaccine effectiveness against severe disease/hospitalisation against Delta and even 80% after just 1 dose.
Though *much less preferable* immunity after infection appears comparable.
PHE analysis suggests 96% vaccine effectiveness against severe disease/hospitalisation against Delta and even 80% after just 1 dose.
Though *much less preferable* immunity after infection appears comparable.
Still ~25k cases/day in 🏴, demonstrating the v high transmissibility of Delta and practically unreachable 'herd immunity threshold'
Despite infections & 'waves' the vax have drastically cut the link w/ hospitalisation so much so it's no longer a systemic risk
via @VictimOfMaths
Despite infections & 'waves' the vax have drastically cut the link w/ hospitalisation so much so it's no longer a systemic risk
via @VictimOfMaths

Can't stress benefits of vax enough!
They protect you and those close to you
And your immunity protects those with weaker immune systems
They protect NHS capacity so we can treat other non covid patients too
They boost freedom by making restrictions and lockdowns unnecessary.
They protect you and those close to you
And your immunity protects those with weaker immune systems
They protect NHS capacity so we can treat other non covid patients too
They boost freedom by making restrictions and lockdowns unnecessary.
• • •
Missing some Tweet in this thread? You can try to
force a refresh