
The @GoggleDocs takeover of @cardiomet_CE continues!
We are 4 UK 🇬🇧 based doctors working across healthcare
Our interests are "what's new, and meaningful in cardiorenal metabolic medicine"
Check out our YouTube channel youtube.com/c/GoggleDocs
We are 4 UK 🇬🇧 based doctors working across healthcare
Our interests are "what's new, and meaningful in cardiorenal metabolic medicine"
Check out our YouTube channel youtube.com/c/GoggleDocs

Yesterday we had key messages from the seminal EMPEROR-Preserved trial✅ & EMPEROR-Pooled analysis✅ presented at the #ESCCongress2021
Today we have key messages from the FIGARO-DKD study & FIDELITY meta-analysis exploring the use of finerenone in T2D & a wide range of CKD
Today we have key messages from the FIGARO-DKD study & FIDELITY meta-analysis exploring the use of finerenone in T2D & a wide range of CKD

Let's start with some background - for starters what in the earth is finerenone?!
Finerenone is a selective non-steroidal mineralocorticoid receptor antagonist (MRA) with different pharmacokinetics & clinical effects to steroidal MRAs such as spironolactone
Finerenone does not sig lower BP & has fewer steroidal effects such as gynaecomastia but can cause ⬆️K+
Finerenone does not sig lower BP & has fewer steroidal effects such as gynaecomastia but can cause ⬆️K+

Finerenone has recently been approved by the @US_FDA as Kerendia to reduce the risk of kidney function decline, kidney failure, CV death, non-fatal heart attacks & hospitalisation for heart failure in adults living with CKD associated with T2D

@US_FDA approval was based on results of FIDELIO-DKD which had 1º renal & 2º CV endpoints
It explored the use of finerenone in people with CKD stage 3 or 4 & severely elevated albuminuria & T2D
Have a look at the earlier tweetorial for a summary
It explored the use of finerenone in people with CKD stage 3 or 4 & severely elevated albuminuria & T2D
Have a look at the earlier tweetorial for a summary
https://twitter.com/cardiomet_CE/status/1389137724926570496

We will give you a bit of time to digest that previous tweetorial! Stay tuned for a discussion of FIGARO and how it links up with FIDELIO
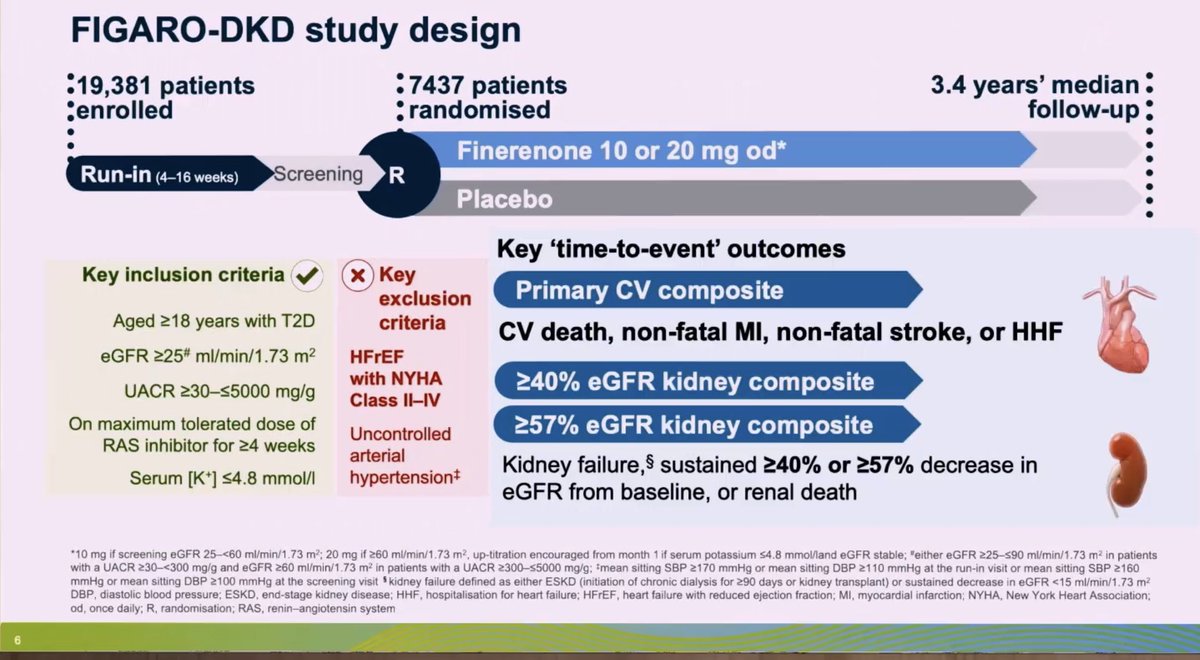
FIGARO-DKD explored the impact of finerenone in people with T2D & a wider range of CKD
In contrast to FIDELIO-DKD, FIGARO-DKD had 1º CV & 2º renal endpoints but less advanced CKD
Nearly half had microalbuminuria and the mean eGFR was 68ml/min
Mean follow-up was 3.4 years
In contrast to FIDELIO-DKD, FIGARO-DKD had 1º CV & 2º renal endpoints but less advanced CKD
Nearly half had microalbuminuria and the mean eGFR was 68ml/min
Mean follow-up was 3.4 years
@drpatrickholmes @AmarPut @dr_amritlamba So, who was studied?
✅7437 participants T2D & CKD
✅ACR 30-300mg/g (microalbuminuria) & eGFR 25-90ml/min (CKD 2-4)
✅ACE 300-5000 (macroalbuminuria) & eGFR at least 60ml/min (CKD stage 122) This group has not been extensively studied in the past
✅ Max tolerated RAS inhibitor
✅7437 participants T2D & CKD
✅ACR 30-300mg/g (microalbuminuria) & eGFR 25-90ml/min (CKD 2-4)
✅ACE 300-5000 (macroalbuminuria) & eGFR at least 60ml/min (CKD stage 122) This group has not been extensively studied in the past
✅ Max tolerated RAS inhibitor
Individuals had to have a K ≤4.8mmol/l at screening
Mean HbA1c 7.7% Mean SBP 136mmHg
Of note, there was 8.4% background SGLT2 inhibitor use & 7.5% background GLP-1 receptor agonist use
These agents have been recommended to reduce cardiorenal risk in many guidelines for T2D
Mean HbA1c 7.7% Mean SBP 136mmHg
Of note, there was 8.4% background SGLT2 inhibitor use & 7.5% background GLP-1 receptor agonist use
These agents have been recommended to reduce cardiorenal risk in many guidelines for T2D

Individuals like those recruited to FIDELIO-DKD i.e., advanced CKD were excluded from FIGARO-DKD
Additionally, individuals with symptomatic HFrEF were also excluded as MRA antagonists are a key pillar of HFrEF management with prognostic and symptomatic benefit
Additionally, individuals with symptomatic HFrEF were also excluded as MRA antagonists are a key pillar of HFrEF management with prognostic and symptomatic benefit

🔵The 1º endpoint of FIGARO-DKD was a composite of death from CV causes, nonfatal MI, nonfatal stroke, or hospitalisation for HF
🔵The key 2º endpoint was a composite of kidney failure, a sustained decrease from baseline of at least 40% in the eGFR, or renal death
🔵The key 2º endpoint was a composite of kidney failure, a sustained decrease from baseline of at least 40% in the eGFR, or renal death

🔥The 1º composite endpoint was significantly reduced by 13% (ARR 1.8%) mainly driven by a 29% RRR in HHF
Other components of 1º endpoint were not significantly reduced
CV benefits were seen in all categories of UACR & eGFR Benefits were also independent of SGLT2i & GLP1RA use
Other components of 1º endpoint were not significantly reduced
CV benefits were seen in all categories of UACR & eGFR Benefits were also independent of SGLT2i & GLP1RA use

The 2º composite renal outcome was numerically lower but did not reach statistical significance
There was no significant difference in adverse events (including AKI & gynaecomastia) between groups
But incidence of ⬆️K+-related discontinuation was ⬆️ with finerenone (1.2%) than placebo (0.4%)
This is less than the expected ⬆️K+ with steroidal MRAs in a similar population
But incidence of ⬆️K+-related discontinuation was ⬆️ with finerenone (1.2%) than placebo (0.4%)
This is less than the expected ⬆️K+ with steroidal MRAs in a similar population
One of the main limitations of FIGARO-DKD was that only around 3.5% of trial participants were of Black ethnic origin
It is well established that individuals of a Black ethnic background are at increased risk of developing end-stage renal disease
It is well established that individuals of a Black ethnic background are at increased risk of developing end-stage renal disease

A pre-specified meta-analysis of individual patient data from FIDELIO-DKD & FIGARO-DKD was presented at the virtual #ESCCongress2021
🔥the FIDELITY analysis!
🔥the FIDELITY analysis!

FIDELITY had 13171 participants of which around 40% had albuminuric CKD with relatively preserved kidney function (mean eGFR 58ml/min)
FIDELITY found that finerenone significantly ⬇️ the risk of a composite CV outcome (time to CV death, nonfatal MI, nonfatal stroke or HHF) by 14%
Finerenone also sig ⬇️ the risk of a composite renal outcome (≥57% decline eGFR, time to kidney failure or renal death) by 23%
Finerenone also sig ⬇️ the risk of a composite renal outcome (≥57% decline eGFR, time to kidney failure or renal death) by 23%

So where does finerenone currently fit into our treatment armamentarium for the management of T2D & CKD?
Recent @goKDIGO 2020 Diabetes in CKD guidance recommends that SGLT2 inhibitors and RAS blockade are used for most patients with T2D & CKD
Recent @goKDIGO 2020 Diabetes in CKD guidance recommends that SGLT2 inhibitors and RAS blockade are used for most patients with T2D & CKD

@goKDIGO Specifically, @goKDIGO recommends that SGLT2 inhibitors should be initiated when eGFR>30ml/min in T2D & CKD to reduce the risk of CKD progression, heart failure & ASCVD even when blood glucose is already well controlled

Where do you see the positioning of finerenone alongside RAS blockade & SGLT2 inhibitors for the management of T2D & CKD? Please comment below why!
In summary:
Finerenone improved CV outcomes mainly driven by a ⬇️HHF in T2D & less advanced CKD with no sig imbalance in adverse events
The FIDELITY MA demonstrated that finerenone is effective for cardiorenal protection across a wide range of CKD in T2D
Finerenone improved CV outcomes mainly driven by a ⬇️HHF in T2D & less advanced CKD with no sig imbalance in adverse events
The FIDELITY MA demonstrated that finerenone is effective for cardiorenal protection across a wide range of CKD in T2D
FIDELIO-DKD, FIGARO-DKD & the FIDELITY meta-analysis also cements the importance of measuring urinary ACR in people living with T2D and preserved kidney function

Declining eGFR & increasing UACR are independent CV risk factors
Mitigation of other CV risk factors & appropriate use of cardiorenal protective therapies inc SGLT2i's, RAS blockade & now finerenone, can improve both quality & quantity of life of people living with T2D & CKD
Mitigation of other CV risk factors & appropriate use of cardiorenal protective therapies inc SGLT2i's, RAS blockade & now finerenone, can improve both quality & quantity of life of people living with T2D & CKD

That's all for today folks! Join @GoggleDocs again tomorrow for the last day of our @cardiomet_CE takeover for more key take-home messages from #ESCCongress2021
• • •
Missing some Tweet in this thread? You can try to
force a refresh












