
1. The face shield (used by medical professional on top of PPEs) in that study are different from the face shields that Filipinos are using. 

2. The virus and the droplets evidently still lingered in the air pointed out by this study. (Probably waiting to be sucked by the suction mechanism brought by a person moving with face shields on)

3. Bartels et al. (2021) pointed out that even though barriers and shields protect people at initial impact of the emission, the droplets will linger for some time due to the constriction brought by the barriers/shields. The study also observed slow settling velocities.

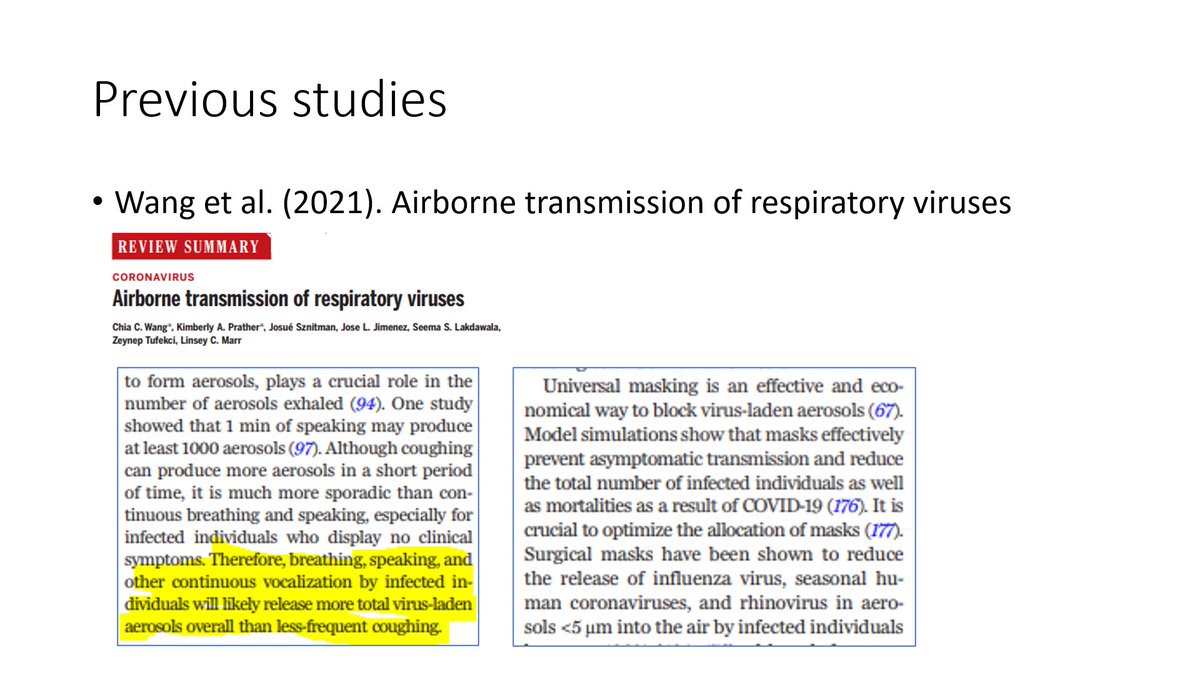
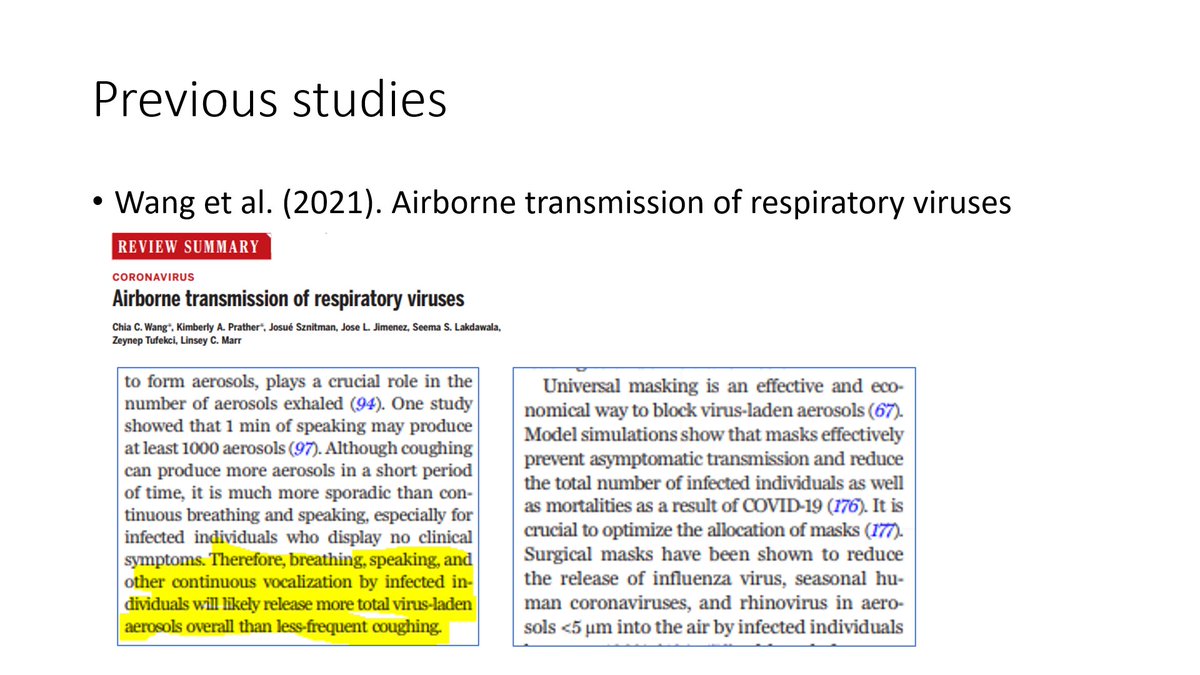
4. In contrast to the setup of Wendling et al. (2021) where the simulated scenario was a short but intense exposure condition, Wang et al. (2021) pointed out that the non-sporadic releases like breathing and speaking releases more virus hence low-momentum scenarios are concerning
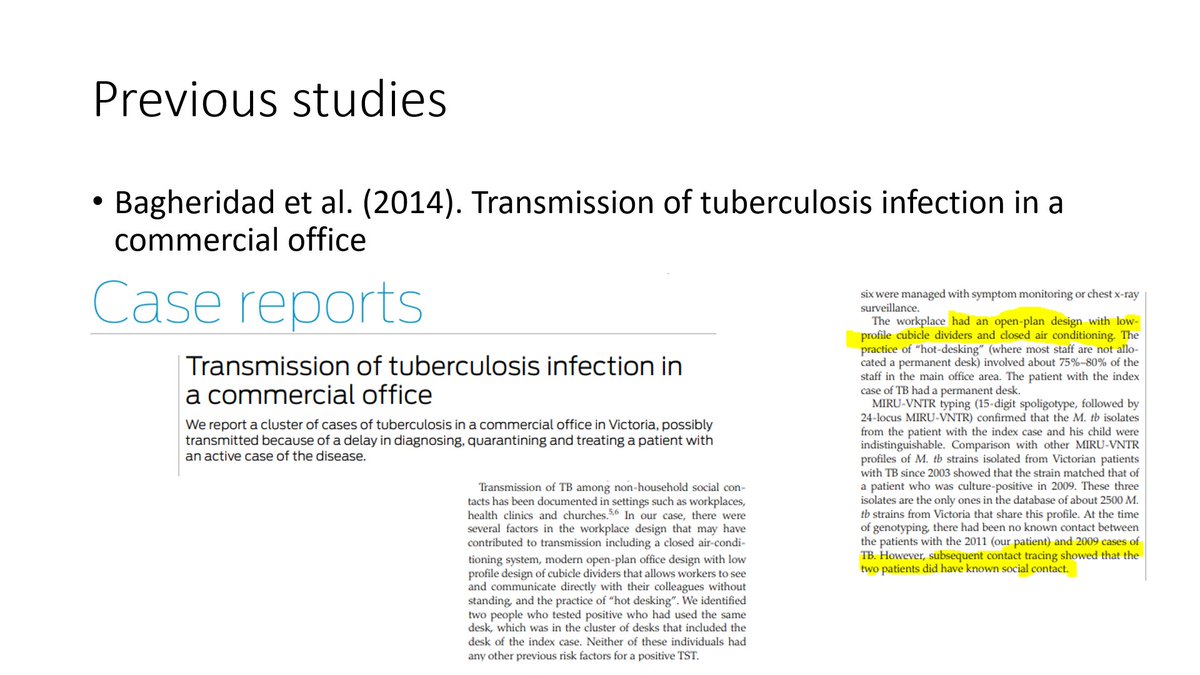
5. Bagheridad et al. (2014) detailed a case study where the barriers of the office cubicles actually allowed the airborne tuberculosis bacteria from an infected worker to linger longer to infect the worker who occupied the cubicle that the infected worker vacated.
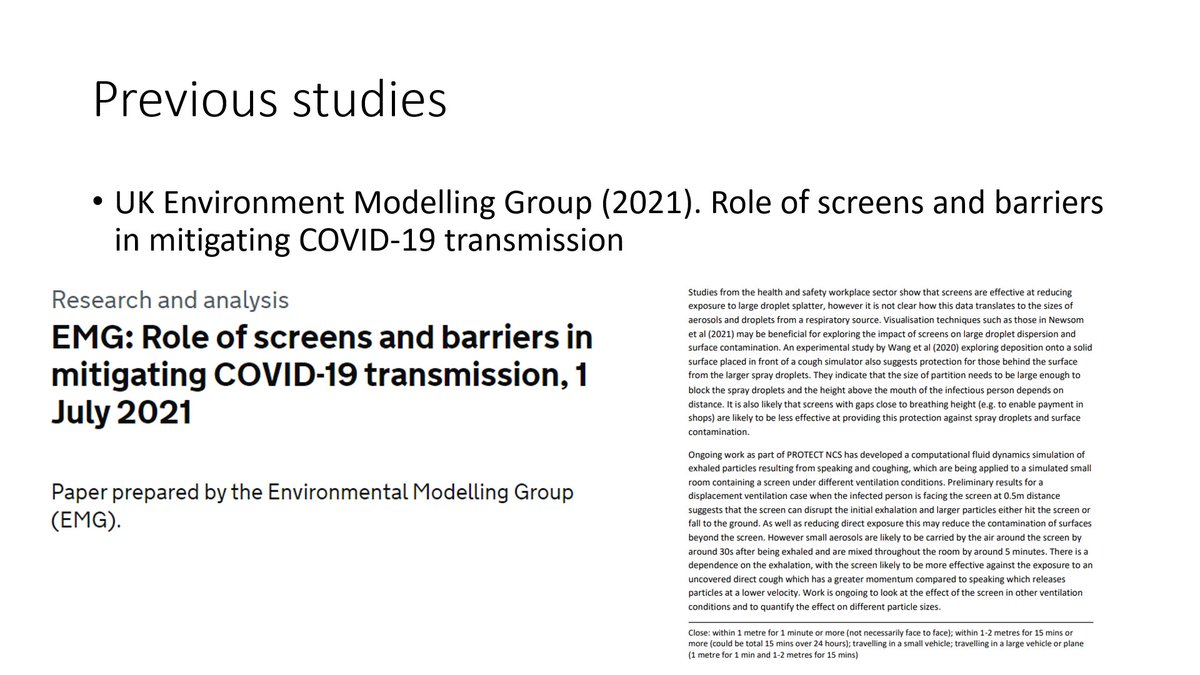
6. The UK Environment Modeling Group (2021) also assessed that constriction of the flow around an enclosed space allows the viruses/particles to linger longer. These actually create dead zones where viruses linger and nestle.
7. And finally, if I were to offer some engineering advice, universal masking was already proven to be effective enough: Engineers would recommend:
(1) What is already enough.
(2) What is also accessible for the use of many.
Spend tons for an extra 1%? Is he out of his mind?
(1) What is already enough.
(2) What is also accessible for the use of many.
Spend tons for an extra 1%? Is he out of his mind?
And to throw back the question I was often asked about (which led me into simulating some more cases): indeed, Wendling et al.(2021) did the scenario where the person at risk is directly facing the source, how about the instances where the person was facing sideways or opposite?
• • •
Missing some Tweet in this thread? You can try to
force a refresh

















