
Time for part 4️⃣ of my comparative physiology series:
Case 1
You are called about an elevated blood alcohol level in an inpatient.
"That’s impossible," the tech says, "he’s been admitted to the ICU for a month!"
It’s totally normal, you say, because the sample came from a __
1/
Case 1
You are called about an elevated blood alcohol level in an inpatient.
"That’s impossible," the tech says, "he’s been admitted to the ICU for a month!"
It’s totally normal, you say, because the sample came from a __
1/
Answer: 🐠
Under anoxic conditions vertebrates produce lactate. This accumulates causing acidosis.
Goldfish & carp are unique b/c they can convert lactate to ethanol, which diffuses out of their gills into the water. They can survive w/o O2 for months!
nature.com/articles/s4159…
2/
Under anoxic conditions vertebrates produce lactate. This accumulates causing acidosis.
Goldfish & carp are unique b/c they can convert lactate to ethanol, which diffuses out of their gills into the water. They can survive w/o O2 for months!
nature.com/articles/s4159…
2/


Other answers
Bats & primates are good ethanol metabolizers by necessity due to a diet that includes fermented fruit.
The Pen Tailed Shrew is an especially fast ethanol metabolizer: adjusted for size, it consumes the equivalent of 9 beers/day!
3/
Bats & primates are good ethanol metabolizers by necessity due to a diet that includes fermented fruit.
The Pen Tailed Shrew is an especially fast ethanol metabolizer: adjusted for size, it consumes the equivalent of 9 beers/day!
3/


In contrast to the shrew, the 🐘 is a very slow EtOH metabolizer due to a loss of the AHD7 gene. Despite their size, elephants can get drunk easily if they eat fermented fruit…which they do.
Pound per pound, a 🐁 could drink an 🐘 under the table!
biotechniques.com/veterinary-sci…
4/
Pound per pound, a 🐁 could drink an 🐘 under the table!
biotechniques.com/veterinary-sci…
4/

Clinical 🥡:
Rarely, humans produce EtOH too. Unlike goldfish (who do it endogenously) in humans it occurs due to abnormalities in gut flora, which ferment sugars into EtOH. This is called auto-brewery syndrome (ABS) & cam occur after a high carb meal.
bmjopengastro.bmj.com/content/6/1/e0…
5/
Rarely, humans produce EtOH too. Unlike goldfish (who do it endogenously) in humans it occurs due to abnormalities in gut flora, which ferment sugars into EtOH. This is called auto-brewery syndrome (ABS) & cam occur after a high carb meal.
bmjopengastro.bmj.com/content/6/1/e0…
5/
Case 2:
Which of these patients would be *MOST* likely to need to visit an oncologist:
6/
Which of these patients would be *MOST* likely to need to visit an oncologist:
6/
Answer: Tazmanian Devil
Devils face extinction from a transmissible cancer called Devil Facial Tumor Disease (DFTD)
When one Devil bites another (as they often do) it can transmit tumor cells directly to the other animal
In 2 decades (1995-2015) over 95% of Devils died of DFTD
7/
Devils face extinction from a transmissible cancer called Devil Facial Tumor Disease (DFTD)
When one Devil bites another (as they often do) it can transmit tumor cells directly to the other animal
In 2 decades (1995-2015) over 95% of Devils died of DFTD
7/



A transmissible cancer means that cells from one organism *directly* invade another.
DFTD occurs b/c the Devil's immune systems can’t recognize the tumor as foreign: limited MHC diversity/expression, constricted T-cell repertoire, & PDL1 upregulation.
pubmed.ncbi.nlm.nih.gov/30225648/
8/
DFTD occurs b/c the Devil's immune systems can’t recognize the tumor as foreign: limited MHC diversity/expression, constricted T-cell repertoire, & PDL1 upregulation.
pubmed.ncbi.nlm.nih.gov/30225648/
8/
Clinical 🥡:
Normally the our immune system prevents non-viral clonally transmissible cancers. Normally.
There is a case of a surgeon who cut himself while resecting a sarcoma & went to to develop a genetically identical sarcoma in his finger later.
nejm.org/doi/full/10.10…
9/
Normally the our immune system prevents non-viral clonally transmissible cancers. Normally.
There is a case of a surgeon who cut himself while resecting a sarcoma & went to to develop a genetically identical sarcoma in his finger later.
nejm.org/doi/full/10.10…
9/


Case 3:
Which of these patients would be *LEAST* likely to need to visit an oncologist:
10/
Which of these patients would be *LEAST* likely to need to visit an oncologist:
10/
Answer: 🐀Naked Mole rat
The naked mole rat is remarkable: a cold blooded mammal that is insensitive to cutaneous pain & can live in as little as 5% FiO2 or as much as 80% CO2.
It’s also the longest lived rodent & it probably *NEVER* develops cancer!
nature.com/articles/s4156…
11/
The naked mole rat is remarkable: a cold blooded mammal that is insensitive to cutaneous pain & can live in as little as 5% FiO2 or as much as 80% CO2.
It’s also the longest lived rodent & it probably *NEVER* develops cancer!
nature.com/articles/s4156…
11/


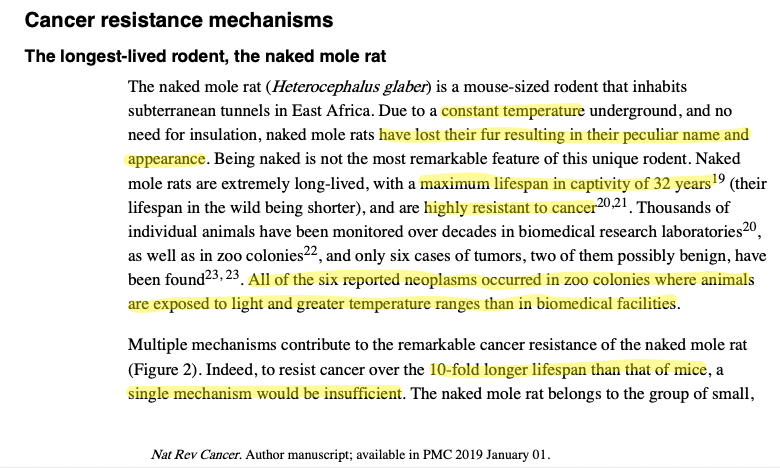
We could (& maybe should) have a whole tweetorial about the naked mole rat, but on the topic of cancer resistance & longevity, there are several mechanisms: a unique ECM matrix & contact inhibition pathways, highly accurate ribosomes, & a low metabolic rate.
12/
12/



Other answers:
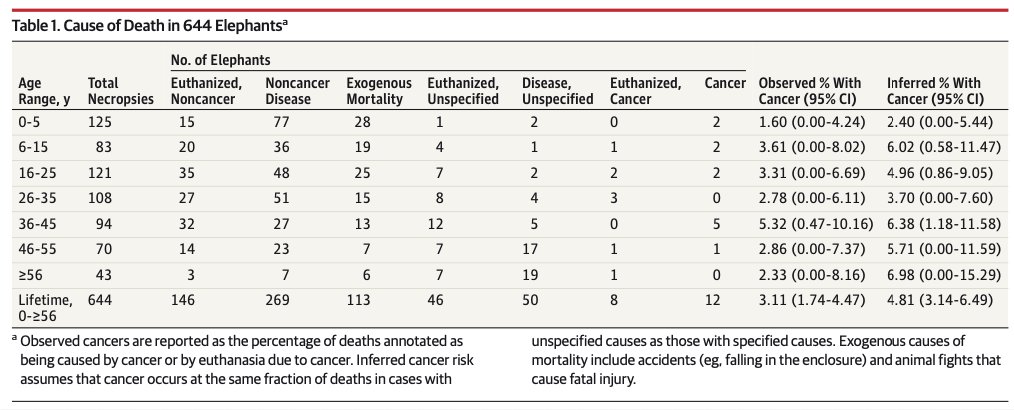
Elephants & bowhead whales are both exceptionally long-lived and highly cancer resistant.
The elephant (lifespan up to 70 years) has 19 additional copies of the p53 tumor suppressor, which makes it highly cancer resistant.
pubmed.ncbi.nlm.nih.gov/26447779/
13/
Elephants & bowhead whales are both exceptionally long-lived and highly cancer resistant.
The elephant (lifespan up to 70 years) has 19 additional copies of the p53 tumor suppressor, which makes it highly cancer resistant.
pubmed.ncbi.nlm.nih.gov/26447779/
13/


The bowhead whale (lifespan >200 years) has enhanced DNA repair mechanisms & upregulates uncoupling protein 1. It likely has novel mechanisms of longevity and cancer resistance that we still don’t comprehend.
ASIDE: There may be bowhead whales that are older than America!
14/
ASIDE: There may be bowhead whales that are older than America!
14/


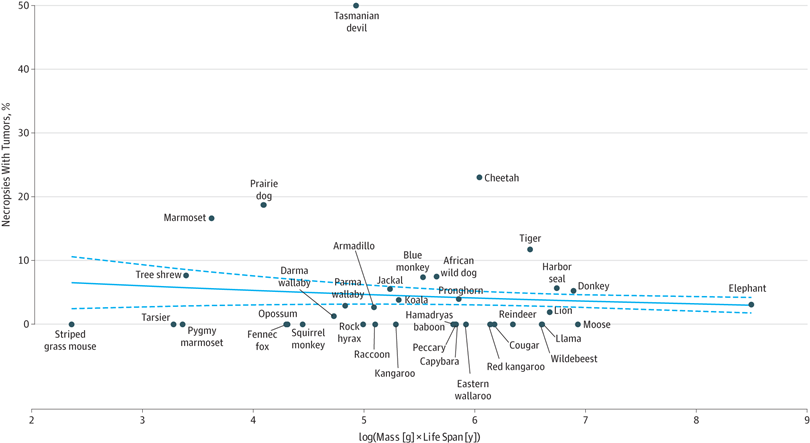
in 1975 Richard Peto observed that despite the fact that humans have 1000x more cells than mice and live 30x longer our risk of cancer is lower. Despite more cells dividing more often, our cancer risk is somehow lower. This is called “Peto’s paradox”
pnas.org/content/116/6/…
15/
pnas.org/content/116/6/…
15/
Clinical 🥡:
There are advantages to having 40 alleles of p53 like elephants do.
Recall that in humans, who have just two copies of p53 (one each from mom & dad), the germline loss of one allele (in Li-Fraumeni syndrome) increases the lifetime risk of cancer to almost 100%.
16/
There are advantages to having 40 alleles of p53 like elephants do.
Recall that in humans, who have just two copies of p53 (one each from mom & dad), the germline loss of one allele (in Li-Fraumeni syndrome) increases the lifetime risk of cancer to almost 100%.
16/
Case 4:
You are called by respiratory therapy about some very weird ventilator settings you ordered:
Tv 55 ml/kg PBW, RR 2, PEEP +5, FiO2 30%
(Yes that really says 55 ml/kg not 5.5!)
You say, it’s OK because the patient is a ___.
17/
You are called by respiratory therapy about some very weird ventilator settings you ordered:
Tv 55 ml/kg PBW, RR 2, PEEP +5, FiO2 30%
(Yes that really says 55 ml/kg not 5.5!)
You say, it’s OK because the patient is a ___.
17/
Answer: Dolphin 🐬
Almost every animal has a tidal volume of ~6 cc/kg PBW.
*The exception is cetaceans (dolphins, whales, porpoises) who need to take much larger breaths more infrequently in order to dive underwater.
18/
Almost every animal has a tidal volume of ~6 cc/kg PBW.
*The exception is cetaceans (dolphins, whales, porpoises) who need to take much larger breaths more infrequently in order to dive underwater.
18/



But *why* is tidal volume constant across (almost) all species?
VO2 increases with size, so alveolar surface area must increase too. Lungs remain about 1% of body weight.
Pressure volume curves are similar across species (the exception is the cat; 🐈s have very stiff lungs!)
19/
VO2 increases with size, so alveolar surface area must increase too. Lungs remain about 1% of body weight.
Pressure volume curves are similar across species (the exception is the cat; 🐈s have very stiff lungs!)
19/


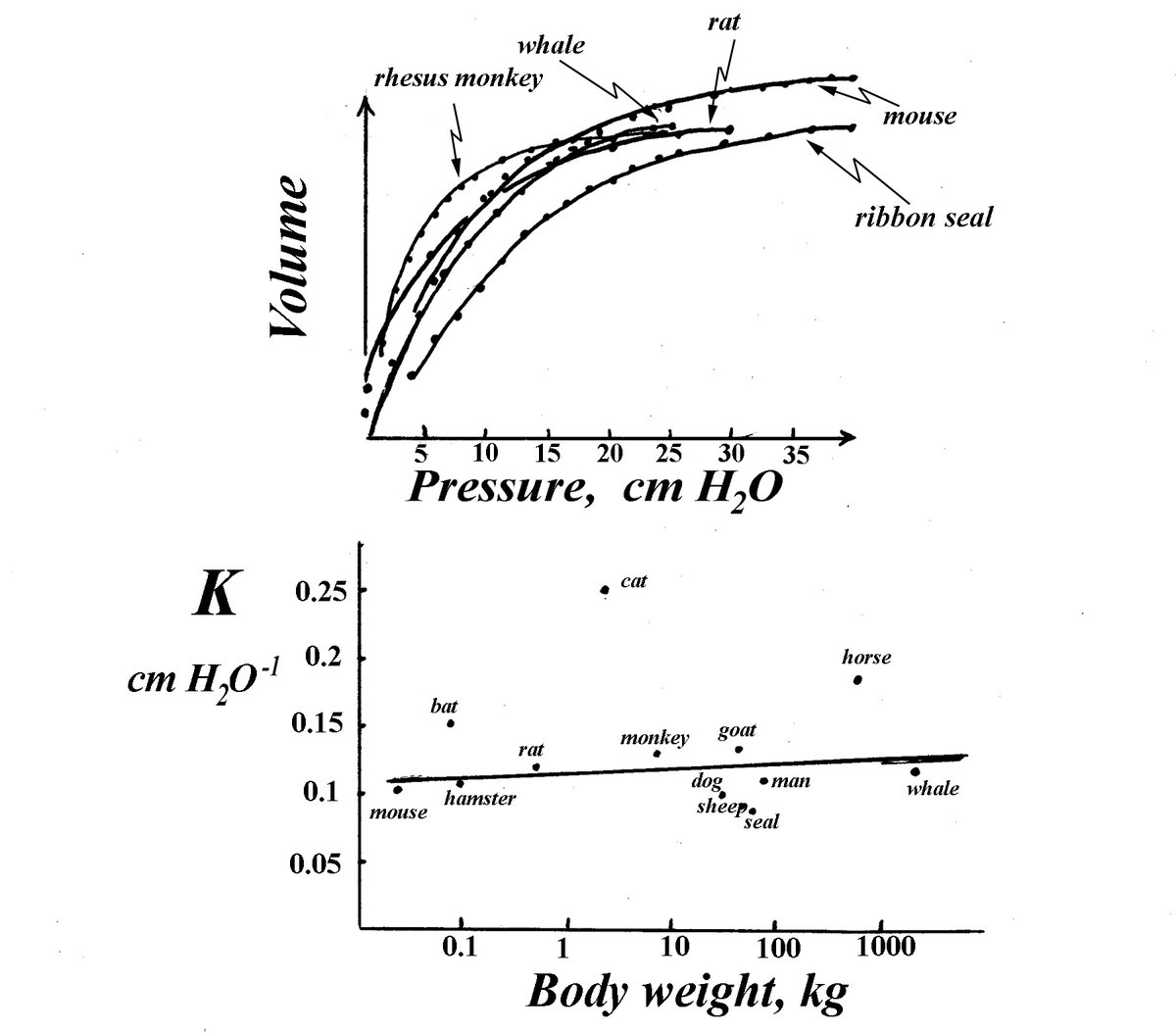

This detail about cat lungs is a bit ironic since this figure (from a 1929 paper by Kurt von Neergaard) is *ALWAYS* used to demonstrate the effect of surfactant on lung compliance, even if it was obtained from “Cat #27”.
H/T to @derangedphys for this.
derangedphysiology.com/main/cicm-prim…
20/
H/T to @derangedphys for this.
derangedphysiology.com/main/cicm-prim…
20/

Also, if you want to learn a lot more about comparative lung physiology I *HIGHLY* recommend this excellent page from McGill. All the graphs, allometric equations, and lung physiology you could possibly want!
medicine.mcgill.ca/physio/resp-we…
21/
medicine.mcgill.ca/physio/resp-we…
21/
Clinical🥡:
That fact that every animal has a TV of 6 cc/kg PBW is a great physiologic basis for “low” tidal volume ventilation, as we use in lung protective ventilation (LPV)
I say “low” b/c a TV of 6 ml/kg PBW really ought to be considered "normal"!
pubmed.ncbi.nlm.nih.gov/24714700/
22/
That fact that every animal has a TV of 6 cc/kg PBW is a great physiologic basis for “low” tidal volume ventilation, as we use in lung protective ventilation (LPV)
I say “low” b/c a TV of 6 ml/kg PBW really ought to be considered "normal"!
pubmed.ncbi.nlm.nih.gov/24714700/
22/


I hope you’ve enjoyed part 4️⃣ of my comparative physiology series.
Thanks to those who suggested topics, the years I spent doing cancer research, & my google news alert about naked mole rats.
If you want more, you can find links to parts 1-3 below:
23/23
Thanks to those who suggested topics, the years I spent doing cancer research, & my google news alert about naked mole rats.
If you want more, you can find links to parts 1-3 below:
23/23
1️⃣
2️⃣
3️⃣
https://twitter.com/nickmmark/status/1346589425938010112?s=20
2️⃣
https://twitter.com/nickmmark/status/1352335092350238721?s=20
3️⃣
https://twitter.com/nickmmark/status/1434137938183344129?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh
































