Crushing chest pain and diaphoresis.
The computer reads "inferior ischaemia"
You, the astute twitter-reading clinician, read "normal"
Here's why 👇🏾🧵
litfl.com/ecg-case-134
The computer reads "inferior ischaemia"
You, the astute twitter-reading clinician, read "normal"
Here's why 👇🏾🧵
litfl.com/ecg-case-134
No, you are not smarter than a computer. But computers don’t allow for human error.
This ECG looks a bit odd. That should prompt us to shift to our system 2 thinking (systematic, conscious, analytical interpretation). (1/11)
This ECG looks a bit odd. That should prompt us to shift to our system 2 thinking (systematic, conscious, analytical interpretation). (1/11)
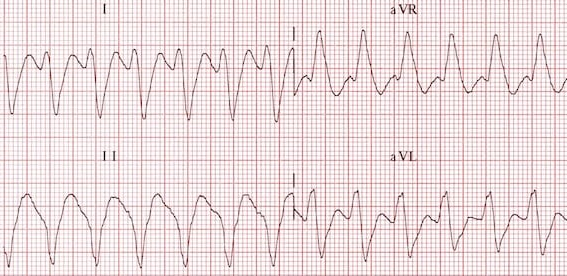
Immediately, we notice an abnormal P wave axis, with an upright P wave in aVR and negative in II.
Whilst on its own this can represent an ectopic atrial rhythm, the QRS axis is also abnormal and is northwest. (2/11)
Whilst on its own this can represent an ectopic atrial rhythm, the QRS axis is also abnormal and is northwest. (2/11)
Our potential causes of a northwest axis include:
- Ventricular rhythms (VT, AIVR, ventricular ectopy)
- Hyperkalaemia
- Extreme RAD
- Dextrocardia
However, QRS conduction itself is normal. (3/11)
- Ventricular rhythms (VT, AIVR, ventricular ectopy)
- Hyperkalaemia
- Extreme RAD
- Dextrocardia
However, QRS conduction itself is normal. (3/11)
A NW axis in hyperK is a relatively late sign – we would expect significant intraventricular conduction delay and an abnormal QRS.
Extreme RAD, usually seen in COPD patients, should be associated with other features of RVH, P pulmonale, and/or arrhythmias such as MAT. (4/11)
Extreme RAD, usually seen in COPD patients, should be associated with other features of RVH, P pulmonale, and/or arrhythmias such as MAT. (4/11)
In dextrocardia, there is absent R wave progression in precordial leads – in fact, there is often R wave REVERSAL as the lateral precordial leads move further away from the right-sided heart. (5/11)

So where does this leave us? Well, a NW axis in an ECG with normal precordial leads simply does not make sense. This must be lead misplacement.
Limb electrode reversal is a common cause of ECG abnormality and can simulate ectopic rhythms, chamber enlargement or ischaemia. (6/11)
Limb electrode reversal is a common cause of ECG abnormality and can simulate ectopic rhythms, chamber enlargement or ischaemia. (6/11)
Recognising this pattern is easier if we understand the changes. Limb leads are calculated from LA, RA, and LL electrodes.
For example, “lead I” = LA – RA, “lead II” = LL – RA, and so forth. (7/11)
For example, “lead I” = LA – RA, “lead II” = LL – RA, and so forth. (7/11)
The relationship between limb leads and electrodes can be described by Einthoven triangle – whilst this diagram can be overwhelming, it gives us an overview of all lead derivations.
Notice how augmented leads such as aVR are simply derived from leads I and II. (8/11)
Notice how augmented leads such as aVR are simply derived from leads I and II. (8/11)
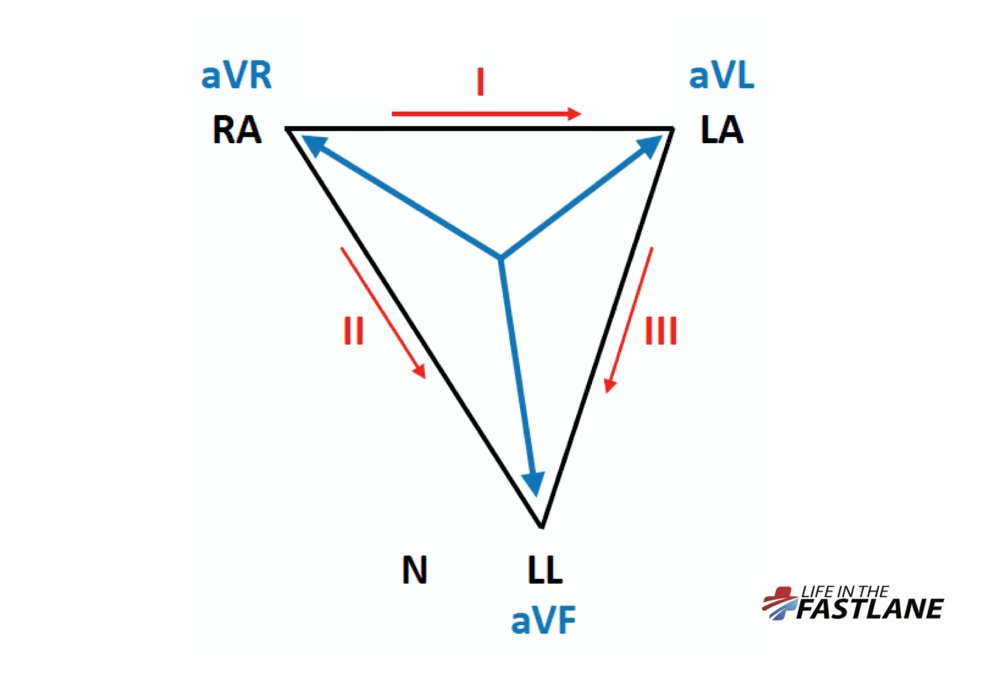
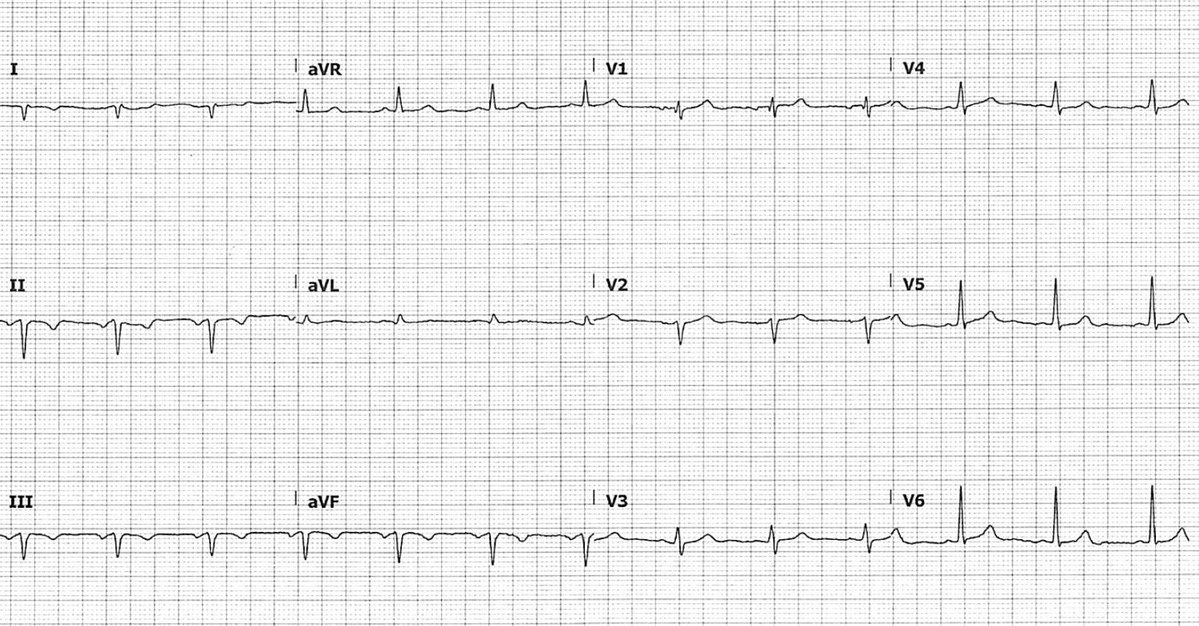
Our patient above has RA/LL electrode reversal. Their "triangle" has been flipped around the fixed LA vector.
Most notably, aVF and aVR switch places. All of leads I, II and III are now "inverted". (9/11)
Most notably, aVF and aVR switch places. All of leads I, II and III are now "inverted". (9/11)

Here is a quick guide to spotting different types of limb lead reversal (10/11)
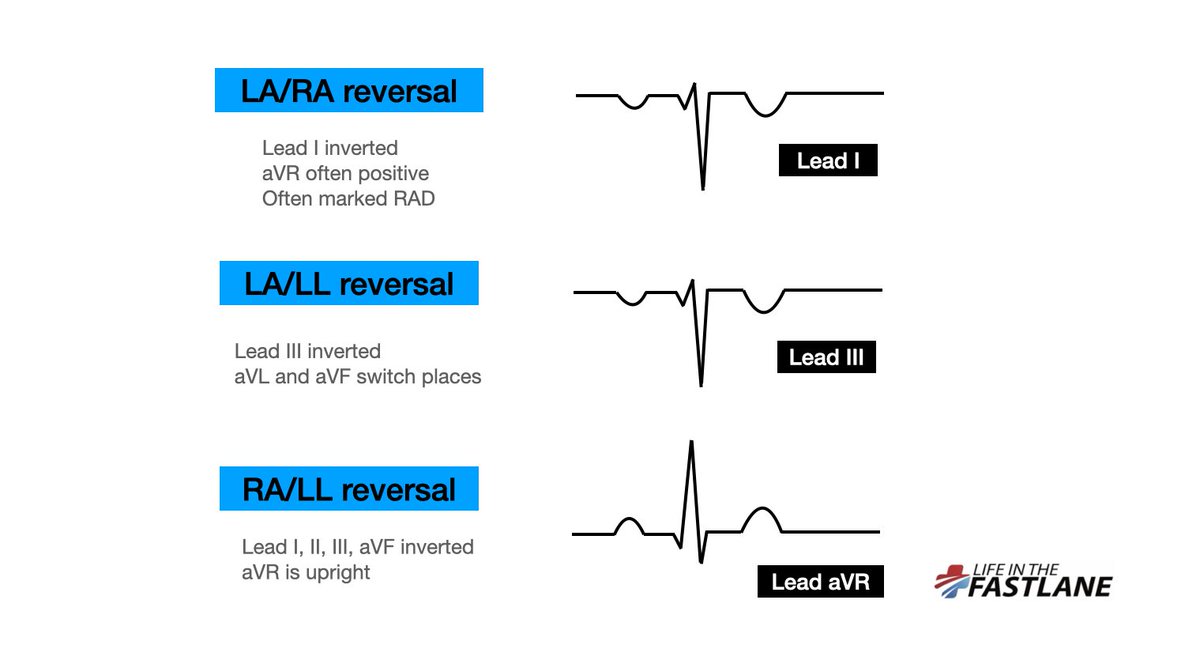
It can be a bit much to remember the exact changes in each type of limb lead reversal.
More relevant is that a uniformally positive aVR, or negative lead I, should always prompt us to consider and check lead reversal, especially when the QRS complex is otherwise normal. (11/11)
More relevant is that a uniformally positive aVR, or negative lead I, should always prompt us to consider and check lead reversal, especially when the QRS complex is otherwise normal. (11/11)
• • •
Missing some Tweet in this thread? You can try to
force a refresh