Short rant on definitions:
I keep getting invitations from researchers who seek to "develop a standardised definition" of X. Such pursuits are usually futile and counterproductive. We need a standardised kilogram but not a standardised way of talking about how the world is.
1/
I keep getting invitations from researchers who seek to "develop a standardised definition" of X. Such pursuits are usually futile and counterproductive. We need a standardised kilogram but not a standardised way of talking about how the world is.
1/
The American Pragmatist Charles Sanders Peirce (thanks for the intro, @MisakCheryl) said “Nothing new can ever be learned by analysing definitions”. Rather, we need to understand how a concept is used and what it contributes to our understanding.
2/
2/
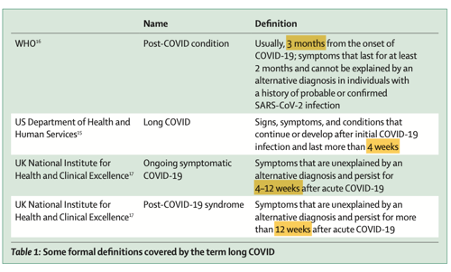
In the context of Covid-19 (to take one complex phenomenon which people seek to rationalise), we need to look at the problem in multiple different ways from different angles.
3/
3/
We won't enrich our understanding by demanding consistent definitions or ways of expressing what are essentially qualitative phenomena. We need deliberation and mutual enlightenment, not technocratic standardisation.
4/
4/
I've just been invited to contribute to the development of a standardised definition of "sustainability", for example. I refused. The term is used by different people in different ways because that's how language works. Plus, meanings *evolve* as our lives and language evolve.
5/
5/
Well-meaning efforts to produce "standard definitions" are also about scientific power. Invite people whose views you value (and, often, share) to contribute to the definition. Bingo, you control how a word gets to be used "correctly" and "incorrectly".
6/
6/
This drive to control our scientific language should not be mistaken for "rigour". It is misguided and potentially sinister. Let's talk about stuff, look at how words and concepts are used in real world settings, and strive for understanding, not control.
7/
end of rant
7/
end of rant
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh