
What about natural immunity? A thread.
I'm not a virologist or vaccinologist. I'm addressing this issue as someone whose career has been focused on plasma cells, the cells that make antibodies, for over 20 years. 👇
I'm not a virologist or vaccinologist. I'm addressing this issue as someone whose career has been focused on plasma cells, the cells that make antibodies, for over 20 years. 👇
1) When first exposed to an antigen, virus or vaccine, the immune system produces a primary immune response. On exposure to same antigen again, it produces a better, bigger, and more durable secondary response. Basic immunology. microbiologynotes.com/differences-be… 

Sometimes the first infection gives a long enough exposure to the antigen to stimulate the secondary response. Sometimes it's not. Depends on the virus and duration of infection.
So even if someone had COVID, it's better to get the vaccine also to ensure a better, durable secondary immune response. More IgG producing cells, more long lived memory cells.
Given the rate of reinfections we are seeing, it is worrying that COVID doesn't seem to produce an enduring immune response in everyone.
It's possible that 2 vaccine doses given too close to each other may also not produce a durable secondary response. (Why some need boosters).
It's possible that 2 vaccine doses given too close to each other may also not produce a durable secondary response. (Why some need boosters).
2) If someone has not yet had Covid, then between getting immunity from the vaccine versus virus, even if the virus induced response is for argument sake better, it is much more risky to acquire immunity that way. It is far safer to get it through a vaccine.
3) Testing for antibodies and then deciding who to vaccinate and who not to is not realistic when we have 70 million eligible left to vaccinate in the US.
4) The virus is also mutating. The more infections we have, the more risk of mutants. Hence the push for vaccinations.
4) The virus is also mutating. The more infections we have, the more risk of mutants. Hence the push for vaccinations.
5) There are side effects with the vaccines as there are with any medicine. But truly serious ones are very rare compared to risk of COVID related complications or death. 215 million people have been vaccinated in the US. 3.75 billion people in the world: Almost half the world.
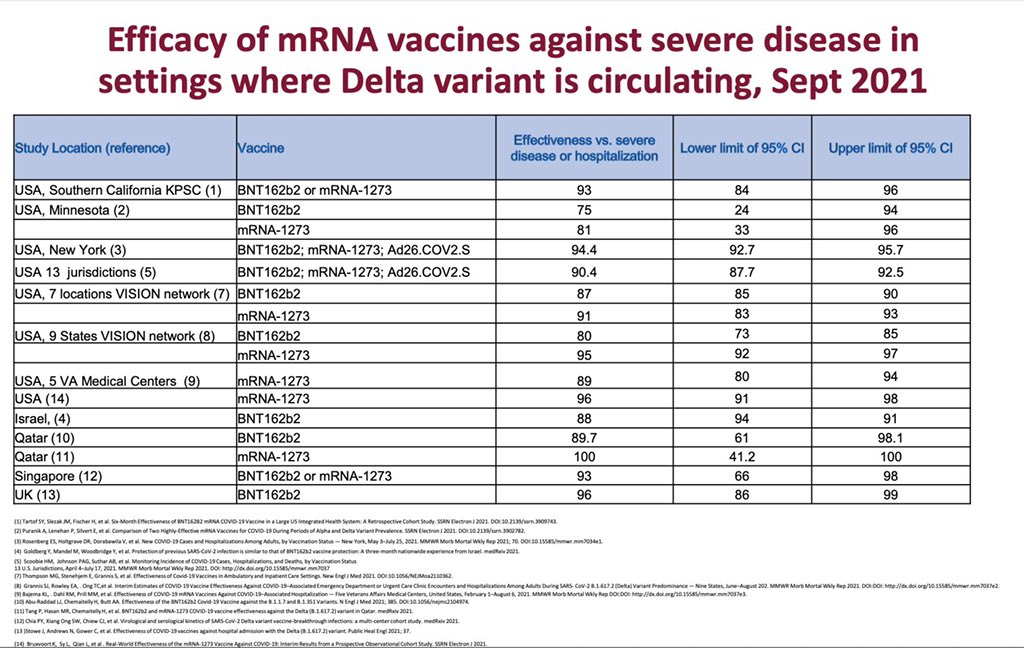
6) There will always be people who doubt the efficacy of vaccines because they hear someone got severe Covid despite vaccines and therefore why bother. Actually vaccines reduce your risk of severe Covid by 90%. They work: Randomized trials and Real world data.
More here on clarifying doubts about vaccine efficacy.
https://twitter.com/VincentRK/status/1409587976544296962
So yeah whether you had COVID or not better to get vaccinated. This is the advise I have given my own family.
Update: We know now from the omicron wave 2 important things.
1) Boosters help. More exposures to same antigen increases protection. Get the booster.
2) Prior Covid "natural immunity" doesn't protect fully. Better to get vaccinated. Including booster. bbc.com/news/health-60…
1) Boosters help. More exposures to same antigen increases protection. Get the booster.
2) Prior Covid "natural immunity" doesn't protect fully. Better to get vaccinated. Including booster. bbc.com/news/health-60…
• • •
Missing some Tweet in this thread? You can try to
force a refresh


















