Starting off day 2 of #CHEST2021 with "Ventilator Basics to Advanced Modes"! 1/
First up is Dr. Amik Sodhi with "The Basics"! #CHEST2021 2/
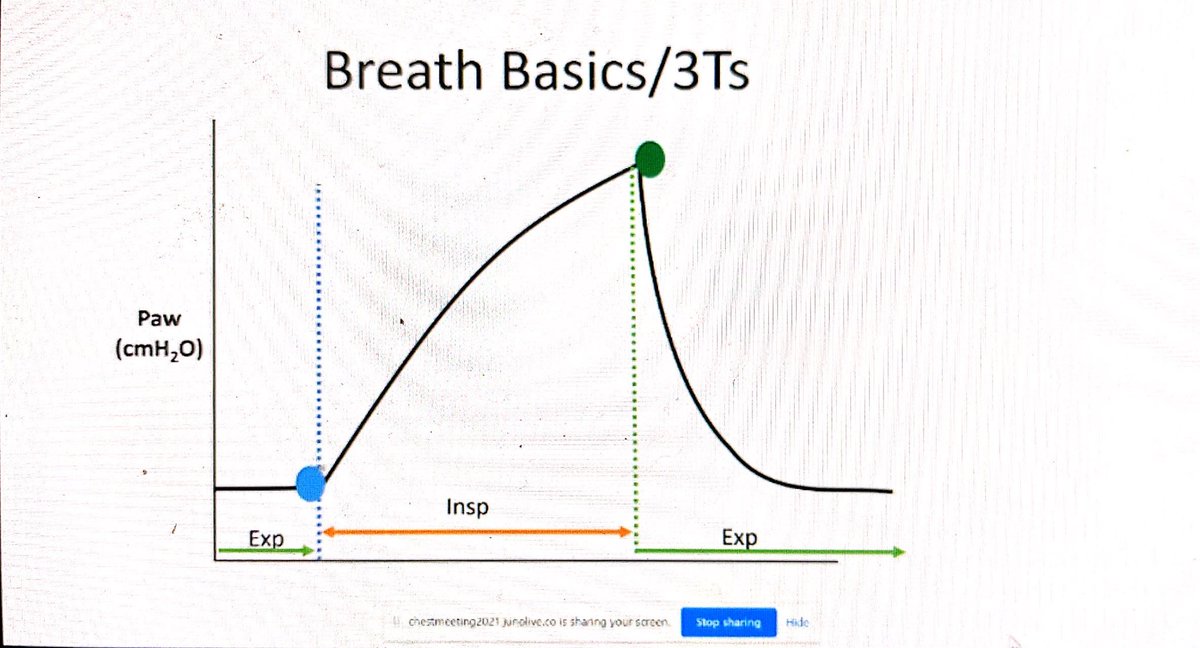
The 3 variables that set a breath are the 3Ts. The trigger is what makes the breath start. The target variable is the breath delivery (something that must be achieved, but not exceeded during the breath. The termination variable is what tells the breath to stop. #CHEST2021 3/ 
In a control breath the vent does all of the work. An assisted breath is started by the patient but finished by the vent. In a supported breath the patient does most of the work. #CHEST2021 4/

Putting these different variables together in different ways determines the vent mode. #CHEST2021 5/

Volume/pressure assist is different from control because the patient triggers the assisted modes. #CHEST2021 6/

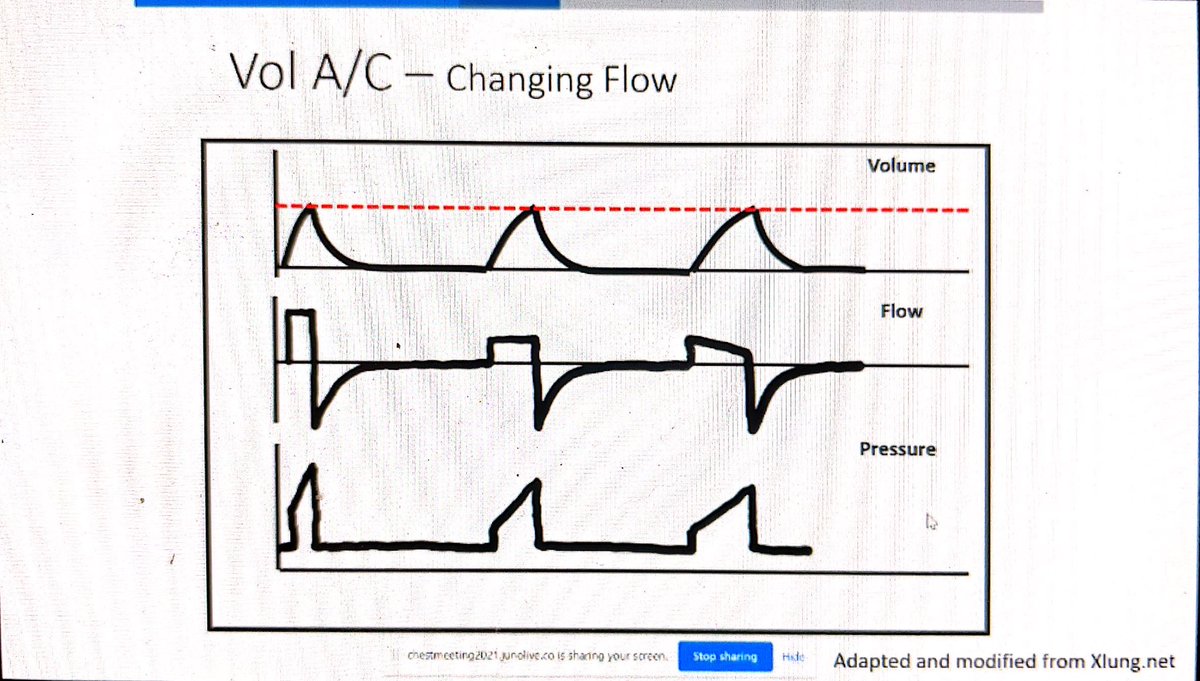
If you have a decelerating flow ramp your time will be longer for the same tidal volume than a square flow. #CHEST2021 7/
An elevated peak pressure with a normal plateau pressure supports a resistive problem. This can also be seen as problems in the expiratory flow curve. #CHEST2021 8/

When the peak and plateau pressures are both high consider compliance problems. #CHEST2021 9/

In pressure A/C remember that your minute ventilation can change a lot with changing compliance. #CHEST2021 10/

If you increase the IP or the inspiratory time you will get an increased TiV. #CHEST2021 11/

Pressure support is totally dependent on the patient's effort. If you decrease the PS the patient will get a smaller volume for the same amount of effort. #CHEST2021 12/

Recruitment is the dynamic process of opening previously collapsed lung units by increasing transpulmonary pressure. #CHEST2021 14/

In a recruiter you will see an increase in the normally aerated lung, whereas a non-recruiter may see an increase in atelectatic and/or overdistended lung tissue with increased pressures. #CHEST2021 15/

Recruitment can be assessed by CT, electrical impedance tomography, and hysteresis. #CHEST2021 16/



A high recruitment-to-inflation ratio can reflect a high potential for reflection. #CHEST2021 17/

Driving pressure (Plateau pressure - PEEP) assessment helps us to minimize VILI. #CHEST2021 18/

Transpulmonary pressure can be measured with an esophageal balloon. Ideally you can use this to set a PEEP that gives you a transpulmonary pressure at end-expiration of 0-5 cm H2O. #CHEST2021 19/

Note that there are many contraindications to recruitment maneuvers. #CHEST2021 20/

Examples of recruitment maneuvers (do not do the third one as it can be harmful). #CHEST2021 21/

Over-distension can worsen lung perfusion because of vessel compression. #CHEST2021 22/

Lung recruitment maneuvers do not improve mortality and they should only be used as a rescue strategy. #CHEST2021 23/

Next up is my dear friend, Dr. Alice Gallo de Moraes (@GallodeMoraesMD) with "Non-Traditional/Advanced Modes". #CHEST2021 24/
APRV is known for being able to maximize recruitment. Longer inspiratory times lead to a higher mean airway pressure and better oxygenation. #CHEST2021 25/

You set APRV by setting a P-high and a P-low. Be careful not to set P-high too high as it can cause overdistension. #CHEST2021 26/
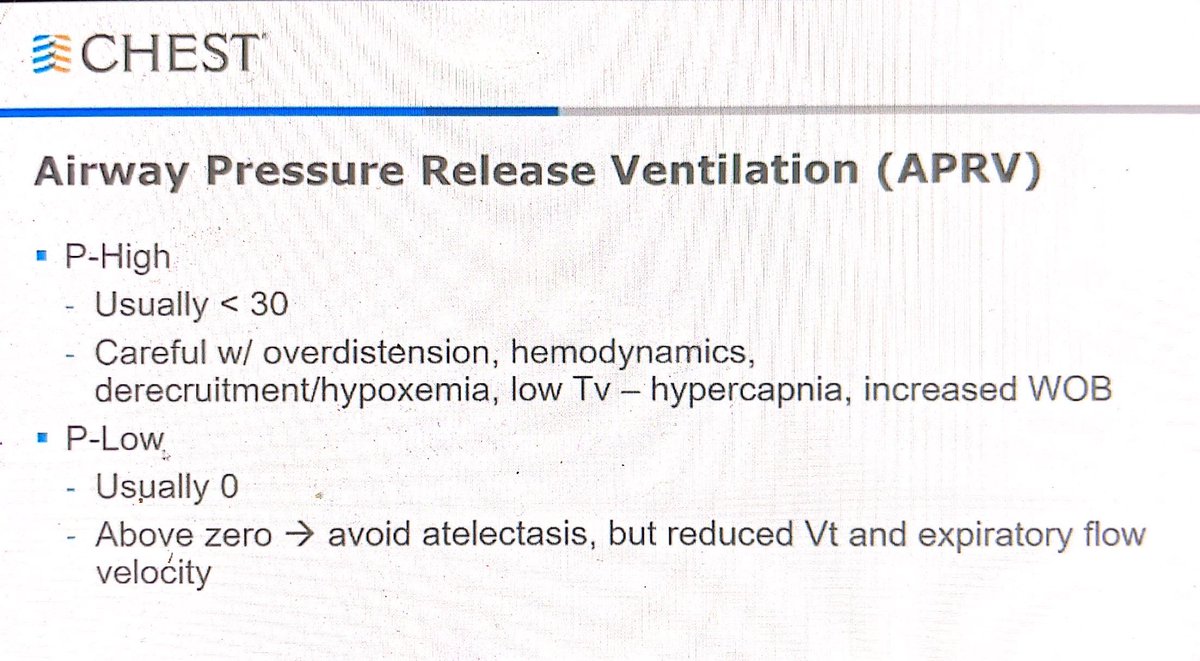
Increased T-high will decrease the release frequency. Too many releases can cause derecruitment and too few can lead to hypercapnea. #CHEST2021 27/
The red line here is the pressure applied by the vent. The yellow line is the trachea; pressure. #CHEST2021 28/

NAVA relied on the electrical activity of the diaphragm to trigger the vent to deliver a breath. It can be hard to control TiV in patients with high respiratory drive. #CHEST2021 29/

The timing and intensity of the diaphragmatic activity determines the timing and intensity of the ventilator's assistance. #CHEST2021 30/

This diagram shows how NAVA works. #CHEST2021 31/

Take home points! Adapt the vent to your patient - not the other way around! #CHEST2021 32/

What is patient ventilator asynchrony? A mismatch between the patient needs and ventilator delivery. #CHEST2021 34/

Asynchrony culprits #CHEST2021 35/

Why is asynchrony bad? #CHEST2021 36/

Types of PVA include trigger-based, flow-based, and cycle-based. #CHEST2021 37/

In an ineffective trigger the patient wants a breath but the vent does not deliver one. #CHEST2021 38/

Ineffective trigger is more common in patients with obstructive processes (intrinsic PEEP makes it worse). #CHEST2021 39/

A double trigger happens when two breaths are triggered and delivered with inadequate expiratory time. #CHEST2021 40/

Auto-trigger happens without patient effort. #CHEST2021 41/

Intrinsic PEEP happens with inadequate expiratory time, worsening airway resistance, and double triggering. #CHEST2021 42/

Flow starvation happens when a patient demands more flow than the vent delivers. #CHEST2021 43/

The flow can be too fast for the patient when the iTime is too little or the pressure rise is too fast. #CHEST2021 44/

Premature cycling happens when the vent wants to stop the breath but the patient wants to keep breathing in. Delayed cycling happens when the vent wants to keep delivering a breath when the patient wants to start exhaling. #CHEST2021 45/

This is an example of delayed cycling. You can see the patient is trying to exhale while the vent is still delivering the breath. #CHEST2021 46/

In this example of premature cycling the patient is trying to breath in during the expiratory loop of the vent. #CHEST2021 47/

Delayed cycling is the most common type of PVA. #CHEST2021 48/

Example of a double trigger and a "too slow" flow asynchrony. #CHEST2021 49/

This example has multiple PVAs. #CHEST2021 50/

Conclusions #CHEST2021 51/

Thanks for joining us for this AWESOME overview of vent settings! #CHEST2021
• • •
Missing some Tweet in this thread? You can try to
force a refresh