
On Jan 24, 2020 @DrEricDing posted a massive warning about the impending pandemic: The Holy Mother of God thread.
"We are now faced with the most virulent virus 🦠 epidemic the world has ever seen," Eric wrote.
As I read his thread again today, all of it has sadly come true
1/
"We are now faced with the most virulent virus 🦠 epidemic the world has ever seen," Eric wrote.
As I read his thread again today, all of it has sadly come true
1/
He wrote:
"possibly an unchecked pandemic that the world has not seen since the 1918 Spanish Influenza. Let’s hope it doesn’t reach that level but we now live in the modern world 🌎 with faster ✈️+ 🚞 than 1918. @WHO and @CDCgov needs to declare public health emergency ASAP!"
2/
"possibly an unchecked pandemic that the world has not seen since the 1918 Spanish Influenza. Let’s hope it doesn’t reach that level but we now live in the modern world 🌎 with faster ✈️+ 🚞 than 1918. @WHO and @CDCgov needs to declare public health emergency ASAP!"
2/
People quarreled with the R0 that was in @DrEricDing's thread, but most epidemiologists and leaders and organizations missed the forest for the trees.
We know what happened since:
240 million cases worldwide
5 million deaths
46 million cases in the US
>750,000 deaths
3/
We know what happened since:
240 million cases worldwide
5 million deaths
46 million cases in the US
>750,000 deaths
3/
It required quite a bit of analysis, judgment, and guts to issue that kind of warning.
Of course people didn't like to hear this kind of prediction. @dwallacewells has written about the criticism and pushback Eric faced. And how few listened.
nymag.com/intelligencer/…
4/
Of course people didn't like to hear this kind of prediction. @dwallacewells has written about the criticism and pushback Eric faced. And how few listened.
nymag.com/intelligencer/…
4/
Looking back it was not one lucky prediction. Throughout the pandemic @DrEricDing has been right numerous times while many other experts who were a lot more optimistic ended up being wrong.
From duration of vaccine efficacy to variants to issue of masks.
5/
From duration of vaccine efficacy to variants to issue of masks.
5/
I remember CDC deciding in June that fully vaccinated can take off their masks. I like many thought it was a reasonable call. Eric disagreed strongly. Turned out he was right.
He is one of the people I'm glad I follow coz he is up to date on everything COVID. Thanks Eric.
6/
He is one of the people I'm glad I follow coz he is up to date on everything COVID. Thanks Eric.
6/
Note that on the day he made the call, Jan 24, 2020 all of Europe had reported 3 cases. US had reported 2 cases. And @OurWorldInData doesn't start tracking till Jan 28, 2020. That's how early this warning was. 

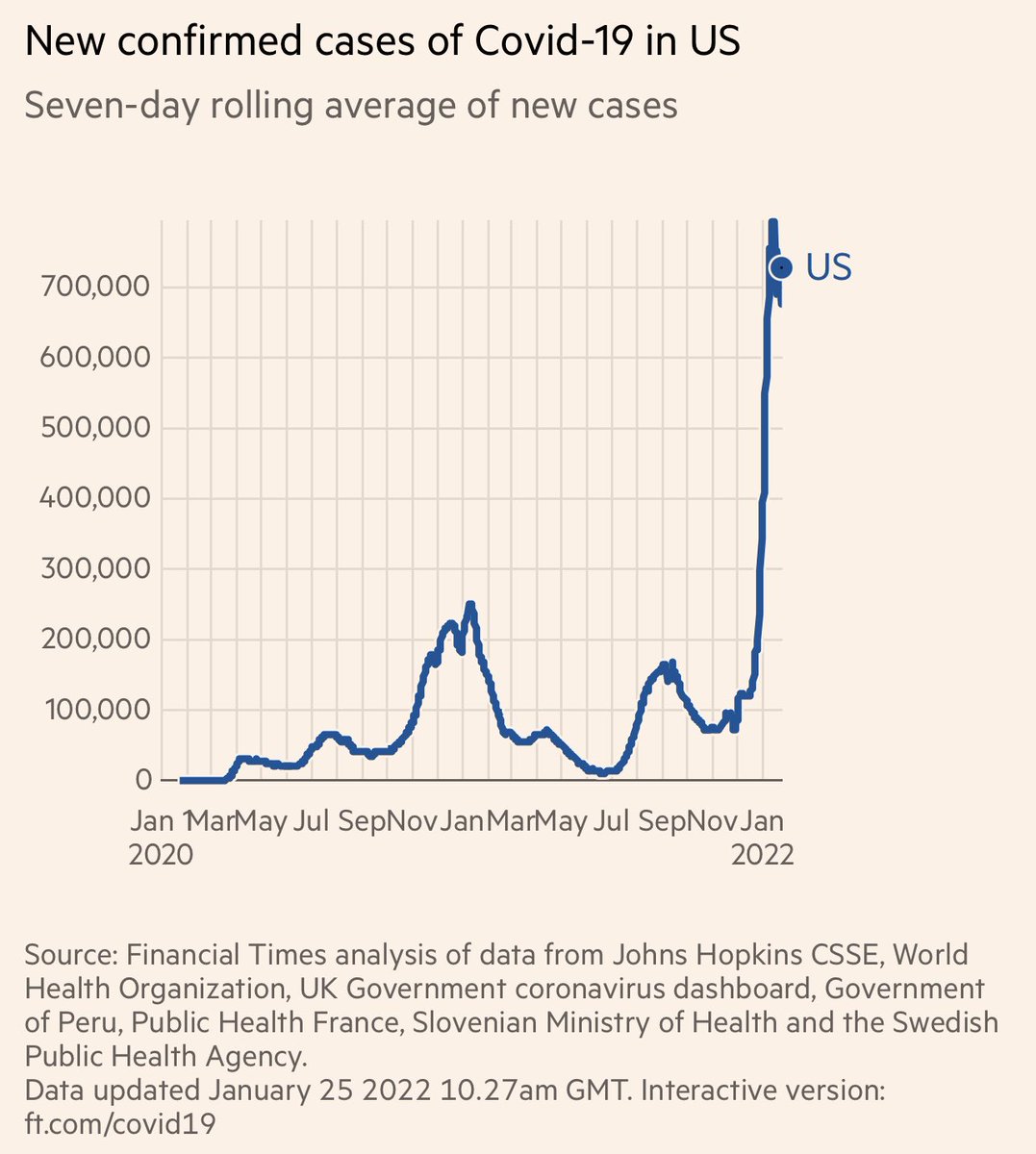
And now, on omicron: On Dec 7, 2021, Eric sounded the alarm that omicron was pandemic 2.0.
A month later, our daily new cases have gone up >4 fold. Hospitals overwhelmed.
A month later, our daily new cases have gone up >4 fold. Hospitals overwhelmed.
https://twitter.com/DrEricDing/status/1468698084632842250
In 45 days, omicron has caused massive problems. With 20 million cases and 60,000 deaths. Pandemic 2.0.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


















