
If you think no one is getting rich off of ivermectin, definitely don't watch this video from FLCCC founder Dr. Fred Wagshul.
For just $276 (cash only, no insurance), this quack will prescribe ivermectin "no questions asked." Don't worry he's got "plenty of product."
Yikes!
1/
For just $276 (cash only, no insurance), this quack will prescribe ivermectin "no questions asked." Don't worry he's got "plenty of product."
Yikes!
1/
His website makes it really clear.
You just fill out this form (including your SSN) and send it to a not at all sketchy gmail address.
Then you pay $211 for a 3 minute phone call and get your prescription. Plus $75 for a followup. Then $75 recurring every 6 months.
2/
You just fill out this form (including your SSN) and send it to a not at all sketchy gmail address.
Then you pay $211 for a 3 minute phone call and get your prescription. Plus $75 for a followup. Then $75 recurring every 6 months.
2/


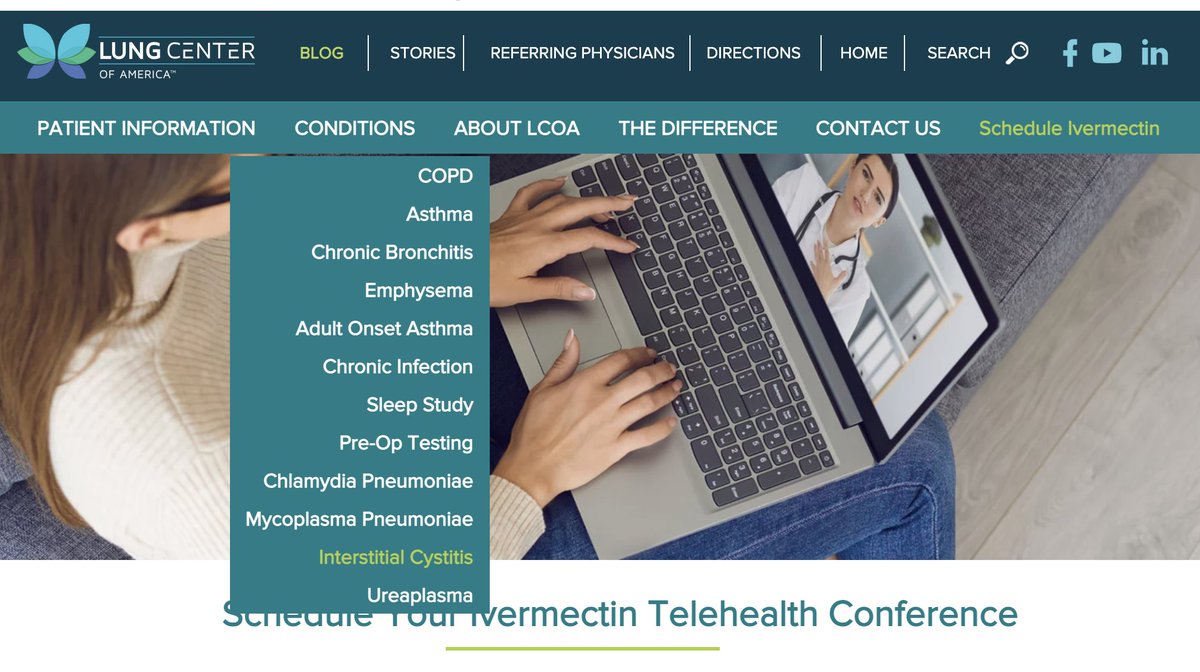
There are quite a few 🚩 on this website.
Aside from referring to $276 telehealth prescriptions for ivermectin as "preventive maintenance" this pulmonologist is also apparently an expert in... interstitial cystitis?
So pulm and urology under one roof. Not at all sketchy.
3/
Aside from referring to $276 telehealth prescriptions for ivermectin as "preventive maintenance" this pulmonologist is also apparently an expert in... interstitial cystitis?
So pulm and urology under one roof. Not at all sketchy.
3/

Also apparently you can get treatment for "overgrowth of normal flora" that doesn't "for most people" doesn't cause any urinary symptoms... sounds like this pulmonary clinic is totally on the up and up.
Just ask all these people hanging out on the beach... in Ohio?
4/
Just ask all these people hanging out on the beach... in Ohio?
4/


But despite weirdly effusive testimonials all over the website... definitely don't ask his clients what they think.
5/
5/




The testimonials on the website (also a big 🚩btw) also suggest quackery:
- patients placed on long standing antibiotics to treat chronic infections
- another person who was “rushed to the hospital and put on an exfoliating mask”
6/
- patients placed on long standing antibiotics to treat chronic infections
- another person who was “rushed to the hospital and put on an exfoliating mask”
6/


Bottom line: sketchy organization (FLCCC) referring patients to a very sketchy doc’s (Washgul) $276 ivermectin teleHealth pill mill.
7/7
7/7
• • •
Missing some Tweet in this thread? You can try to
force a refresh
































