11 November: Non-inferiority, pemetrexed
For Lung Cancer Awareness Month #LCAM I’m going to summarize 30 important lung cancer trials over 30 days. These posts are directed at non-medical professionals, with descriptions of the results and of what makes a good trial. #lcsm 1/11
For Lung Cancer Awareness Month #LCAM I’m going to summarize 30 important lung cancer trials over 30 days. These posts are directed at non-medical professionals, with descriptions of the results and of what makes a good trial. #lcsm 1/11

Today we are back to looking at a study of chemotherapy for metastatic non-small cell lung cancer (NSCLC). Our last study in this area (3 November) established the notion that all platinum doublets were more or less the same. Today’s study, from 2008, overturned that consensus.
This was a trial comparing cisplatin-gemcitabine (standard) with cisplatin-pemetrexed. Pemetrexed is administered in a more convenient schedule than gemcitabine, and likely causes fewer side effects. Because of these advantages, the study was designed for noninferiority. 3/11
This means that the investigators thought they did not have to prove that survival with cis-pem was better, just that it was not substantially worse. This is called a non-inferiority design. Recall our discussion of confidence intervals yesterday. 4/11
The investigators chose a non-inferiority margin of 15%. This choice is arbitrary. The trial is positive if the upper limit of the confidence interval for risk of death with Cis-pem is not 15% worse than the risk with cis-gem. 5/11
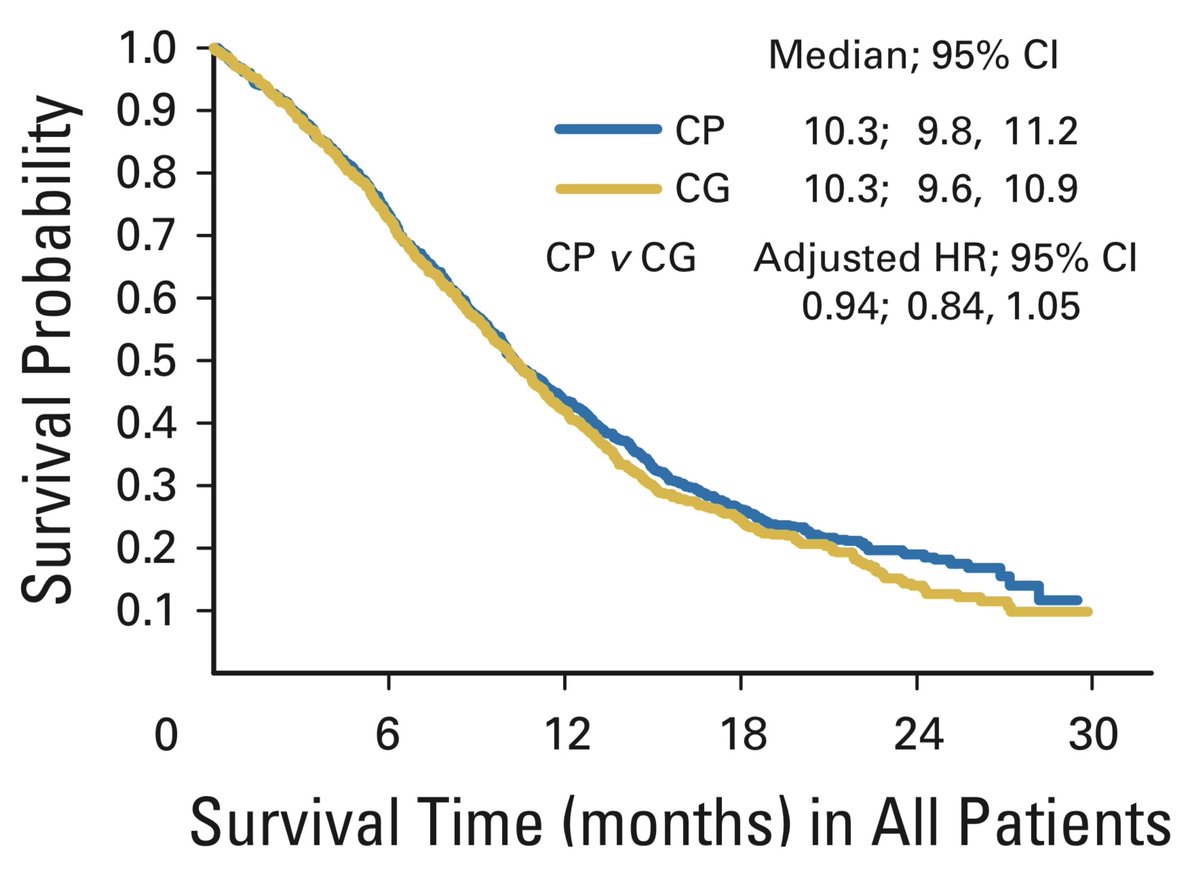
This was a large trial, randomizing 1725 patients. As you can see from the KM curve below, there is no obvious difference between the two arms. Formally, the non-inferiority criterion was met. 6/11
A subgroup analysis was then performed. NSCLC can be divided into subtypes on the basis of the appearance of the cancer cells. Some are squamous carcinoma, others non-squamous (mainly adenocarcinoma). Survival was better with cis-pem in the non-squamous subgroup, but not squamous

This finding has been incredibly influential. Platinum-pemetrexed remains the standard doublet for non-squamous NSCLC to this day. The impact on the sales of pemetrexed has resulted in this being called “The Billion Dollar Subgroup Analysis”. 8/11
Some concerns about this result:
1. The authors performed at least 8 subgroup analyses. Because each has a 5% probability of being positive by chance, the likelihood of a spurious finding is high
2. There was no corresponding PFS advantage with pem, which is hard to explain 9/11
1. The authors performed at least 8 subgroup analyses. Because each has a 5% probability of being positive by chance, the likelihood of a spurious finding is high
2. There was no corresponding PFS advantage with pem, which is hard to explain 9/11

There is no reason to suspect that cis-pem is any worse than other doublets, but the evidence that it is superior to other doublets in non-squamous NSCLC is perhaps not as strong as we’d like to think. We probably put more faith in subgroups than we ought. (See Nov 3, 6, 7...)
Tomorrow is Flower Power, with the FLAURA trial and an introduction to statistical power.
Please, take some time today to observe Remembrance Day. As we mull the cataclysms of the 20th Century may we also find the courage and selflessness to face the cataclysms of the 21st. 11/11
Please, take some time today to observe Remembrance Day. As we mull the cataclysms of the 20th Century may we also find the courage and selflessness to face the cataclysms of the 21st. 11/11

• • •
Missing some Tweet in this thread? You can try to
force a refresh