#lauruslabs
First ever injectable long acting treatment Cabotegravir has got approval from NICE in UK.
This can cause shift in treatment & prophylaxis of HIV and current oral ARV APIs can lose market share in coming years.
nice.org.uk/news/article/n…
First ever injectable long acting treatment Cabotegravir has got approval from NICE in UK.
This can cause shift in treatment & prophylaxis of HIV and current oral ARV APIs can lose market share in coming years.
nice.org.uk/news/article/n…
Recent study published on New England Journal of Medicine has found that Cabotegravir injection(2 monthly) is superior to current ART regimen in pre exposure prophylaxis of HIV in high risk individuals.
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…

Cabenuva annually costs €9824 ($11068).Since it is a 2 monthly injection, only 6 doses are needed annually.
Current treatment regimen in US (Biktarvy) costs $42,000 annually. Comparing to this, Cabotegravir+Rilpivirine is a cheaper.
Current treatment regimen in US (Biktarvy) costs $42,000 annually. Comparing to this, Cabotegravir+Rilpivirine is a cheaper.

Biktarvy is the most prescribed regimen in US with a market share of 41%.
Annual cost of Biktarvy regimen is $42,624. (3552 x 12 = 42,624)
Annual cost of Biktarvy regimen is $42,624. (3552 x 12 = 42,624)


Annual cost for Truvada, another commonly used antiretroviral drug in US is $20,400 (1700 x 12)

This high price is because middle & high income countries are not included in voluntary licensing agreements and they must pay high prices to orginator companies for patented drugs.

Comparing to the current treatment regimen of daily oral intake throughout the lifetime, Cabotegravir+Rilpivirine is only needed to be taken 6 times a year, which provides greater comfort to the patient and reduces social stigma associated with taking ARTs daily.
This helps the patient to adhere to the treatment and reduces suboptimal adherance to ARTs. Unlike current oral therapy injectables also has no gastrointestinal side effects. These factors may compel the ART clinics to shift to newer regimen apart from cheapiness in cost in US.


Injectable Cabenuva has high potential on Pre exposure prophylaxis(PrEP) of HIV infection in high risk individuals (health care workers in HIV management, sex workers,etc). Latest study shown it's superior efficacy over current oral therapy.
Also patients only need to take Inj once in every 2 months unlike current daily dose. In US only less than 25% of target population (high risk individuals) is currently taking PrEP. With this 2 monthly option,more people will opt for it.Viiv expects to make € 2 billion by 2026.

As of now, Laurus labs doesn't develop Cabotegravir API and doesn't have expertise on sterile Injectables.
Revenue from ARV API can drop for Laurus with the shift in the treatment.
Revenue from ARV API can drop for Laurus with the shift in the treatment.
Update on Cabotegravir long acting injectable therapy on LMIC.
You may know that Low income countries get innovator drugs at low cost through licensing agreements made by MPP.
LMIC can get Cabotegravir before patent expiry, at affordable cost if MPP makes deal with innovator.
You may know that Low income countries get innovator drugs at low cost through licensing agreements made by MPP.
LMIC can get Cabotegravir before patent expiry, at affordable cost if MPP makes deal with innovator.
MPP prioritize drugs they need to work on and get deal from the innovator with licensing agreements for the greater good of low middle income countries.

Patented drugs are thus made available on these countries at affordable cost to tackle diseases like HIV, Tb, Hep C.
Their method of prioritizing which drug they need to consider for next deal is based on these 4 factors.
Their method of prioritizing which drug they need to consider for next deal is based on these 4 factors.

Suitable drug candidate for next deal is selected is based on the greatest public health impact the drug can make on the low middle income countries.

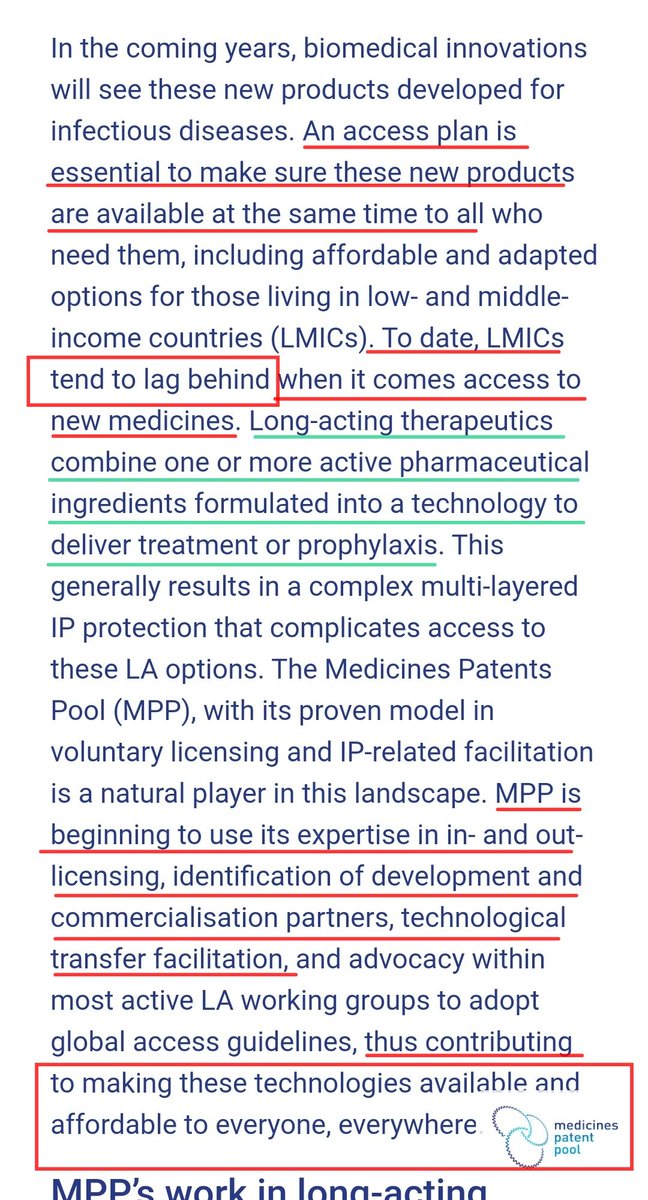
MPP is now considering long acting therapeutics as "game changers in healthcare"
MPP is making an access plan to ensure that these long acting regimens are made available to EVERYONE, EVERYWHERE AT SAME TIME.
MPP is making an access plan to ensure that these long acting regimens are made available to EVERYONE, EVERYWHERE AT SAME TIME.

To date, LMIC tend to lag behind on getting new medicines. MPP is making a plan to change that.
Current HIV priority list of MPP has Cabotegravir long acting injectable and they are monitoring Rilpivirine for prioritizing.
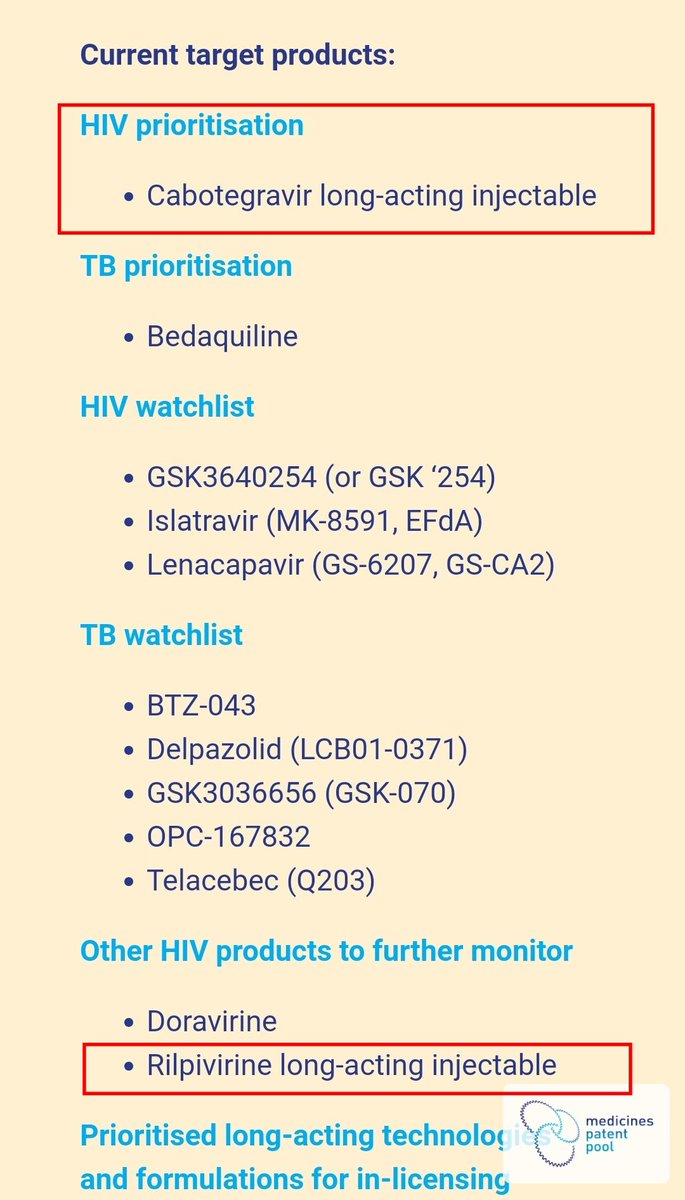
This priority consideration report is from 2020, even before the approval of the drug. We can expect some quick developments from MPP's side as they are quite confident on long acting injectables & consider it as "gamechangers"
Cabotegravir DOESN'T require cold chain.
Cabotegravir DOESN'T require cold chain.

Generally, only vaccines and biological products require cold chain. Sterile small molecules usually doesn't require cold chain.
However 'current formulation' of Rilpivirine requires cold chain.
However 'current formulation' of Rilpivirine requires cold chain.
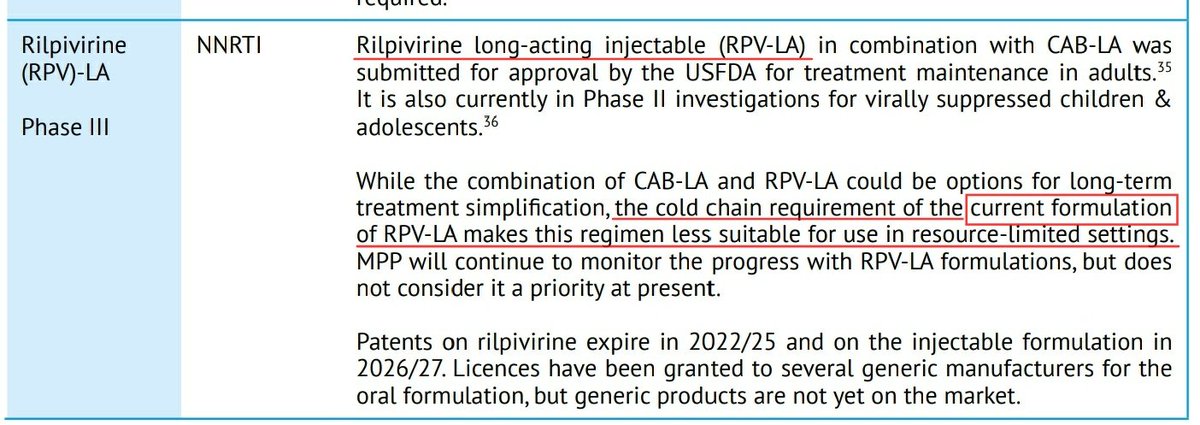
This is because of the nanoparticles which are used to increase the solubility of Rilpivirine. Size and morphology of these nanoparticles changes at room temperature.
However in vivo relevance of this is unknown.
However in vivo relevance of this is unknown.

A pharmacokinetic study is going on to compare the efficay of refrigerated product and aged product(drug which is being kept outside)
So if the efficacy is found to be comparable, we can use Rilpivirine without cold chain requirements.
So if the efficacy is found to be comparable, we can use Rilpivirine without cold chain requirements.

1. So LMIC countries can get Cabotegravir early, if MPP makes a licensing agreement with innovator.
2.MPP has Cabotegravir in their priority list and considers long acting regimen as "gamechanger"
3.MPP is developing access plan to provide innovator drugs to LMIC.
2.MPP has Cabotegravir in their priority list and considers long acting regimen as "gamechanger"
3.MPP is developing access plan to provide innovator drugs to LMIC.
4. Cabotegravir doesn't require cold chain. Rilpivirine may/may not require cold chain.
5. Long acting therapy reduces burden on healthcare system, frees patient from daily pills and helps them stay on treatment.
5. Long acting therapy reduces burden on healthcare system, frees patient from daily pills and helps them stay on treatment.
medicinespatentpool.org/news-publicati…
MPP has signed a licence agreement for an investigational long-acting injectable drug combination candidate for HIV.
“Long-acting technologies are the next frontier for sustained suppression of HIV worldwide, and we are delighted to sign this..."
MPP has signed a licence agreement for an investigational long-acting injectable drug combination candidate for HIV.
“Long-acting technologies are the next frontier for sustained suppression of HIV worldwide, and we are delighted to sign this..."


• • •
Missing some Tweet in this thread? You can try to
force a refresh