
1.Our research team have now analysed the ONS England November mortality data. We conclude that despite seeming evidence to support vaccine effectiveness this conclusion is doubtful because of a range of serious inconsistencies and anomalies.
See: https://t.co/PIkA4fVxBHdx.doi.org/10.13140/RG.2.…

See: https://t.co/PIkA4fVxBHdx.doi.org/10.13140/RG.2.…

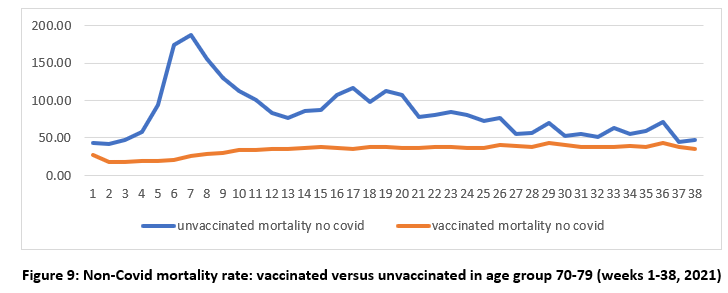
2.The data appear to show lower non-Covid mortality for the vaccinated compared to the unvaccinated. Odd. Also unvaccinated mortality rates peak at the same time as the vaccine rollout peaks for the age group, then falls and closes in on the vaccinated. This is not natural
3. Consider what we are witnessing here. We have a vaccine whose recipients are suffering fewer non-covid deaths and hence are benefitting from improved mortality. And the mortality rates look to differ significantly from historical norms, as evidenced in mortality lifetables.
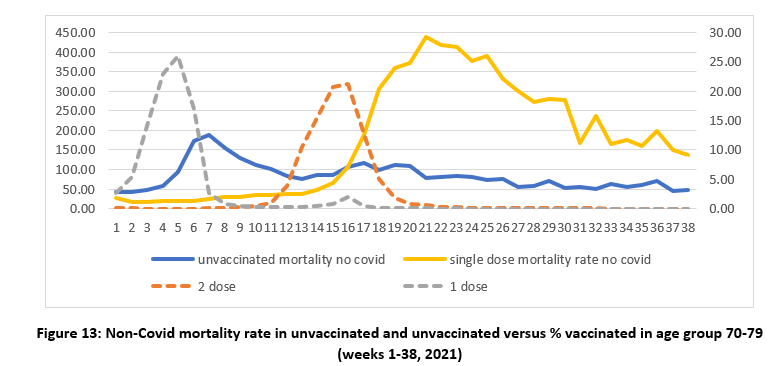
4.Correlating unvaccinated mortality with vaccine roll out we see curious patterns (dotted line the proportion of people getting first and second doses). Why are the unvaccinated dying after NOT getting the 1st dose? Why are the single dosed dying after NOT getting the 2nd dose?
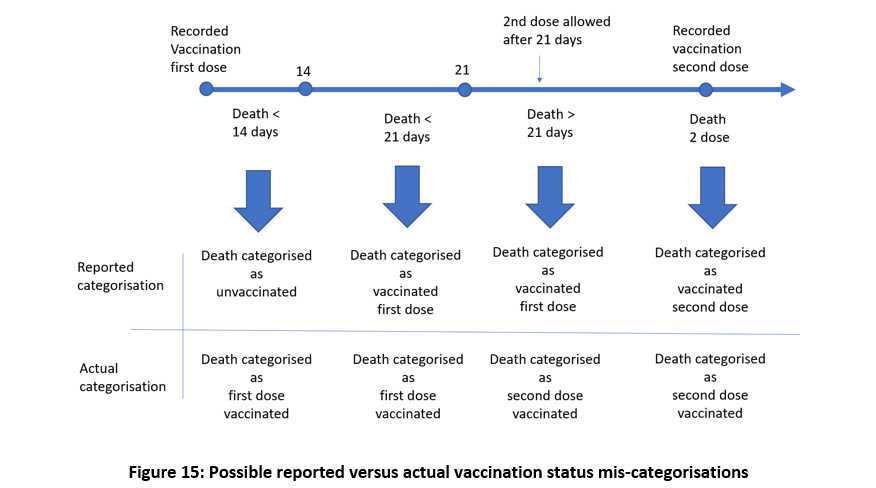
5.Plenty of evidence that the vaccinated who die within 14 days of vaccination may be categorized as unvaccinated. Then someone who dies within 14 days of first dose is miscategorised as unvaccinated and a similar thing could occur post second dose.
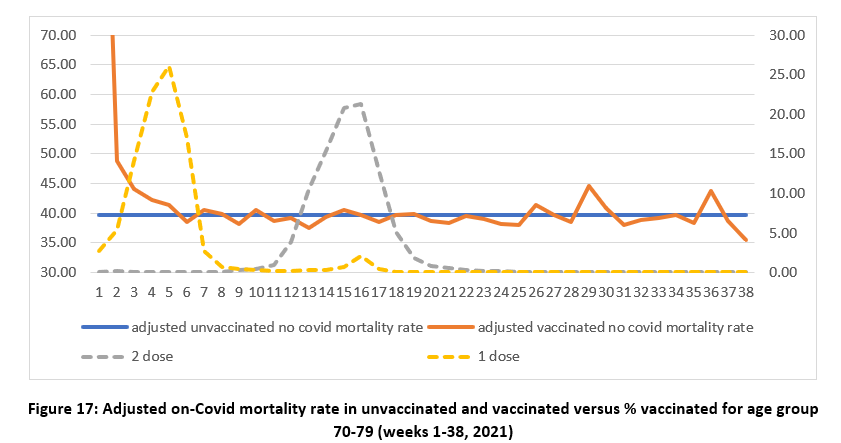
6. Miscategorization might explain odd phenomena in ONS mortality. To correct the error we can take the difference between the expected mortality for the unvaccinated and the data, and re-allocate this unexpected excess mortality to the vaccinated to get new ADJUSTED estimates.
7. The early spikes in mortality that appear to occur soon after vaccination may be caused by the infirm, moribund, and severely ill receiving vaccination in priority order and thus simply appearing to hasten deaths that might otherwise have occurred later in the year.
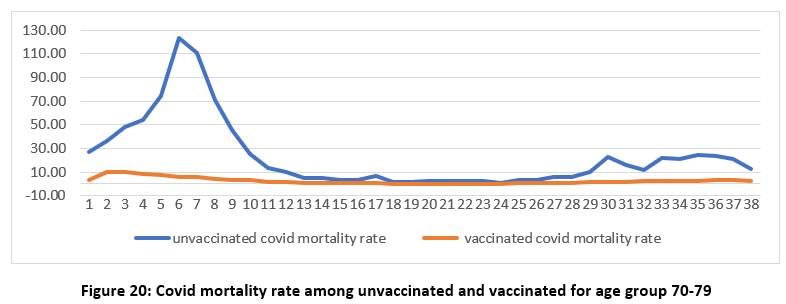
8.Turning to Covid mortality, at face value, there appears to be clear evidence of vaccine effectiveness. But……..
9.After vaccination people endure weakened immune response for a period of up to 28 days and may be in danger of infection from Covid or other infectious agent at any time in that period. It therefore makes sense to examine infection date rather than date of death registration.
10.We adjust for this using a temporal offset and see a large spike in mortality for all age groups during the early weeks, when covid prevalence was high, and when the first dose vaccination rollout peaked.
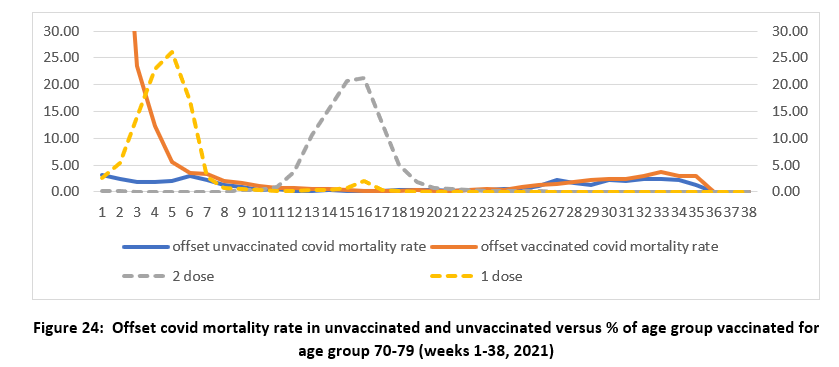
11.After our offset adjustment we observe no significant benefit of the vaccines in the short term. They appear to expose people to an increased mortality, in line with what we know about immune exposure or pre-infection risks,
12.Whatever the explanations for the observed data, it is clear that the ONS data is both unreliable and misleading.
Absent any better explanation Occam’s razor would support our conclusions. The ONS data provide no reliable evidence that the vaccines reduce all-cause mortality.
Absent any better explanation Occam’s razor would support our conclusions. The ONS data provide no reliable evidence that the vaccines reduce all-cause mortality.
Y axis is mortality = deaths per 100,000 of population.
This is the latest of numerous attempt to decode ONS hieroglyphs, but now we may have stumbled upon a rosetta stone to help solve the puzzle.
probabilityandlaw.blogspot.com
probabilityandlaw.blogspot.com
This is unrewarded work done at some considerable career risk.
Some of our clinical collaborators COULD NOT put their names on the paper.
Some of our clinical collaborators COULD NOT put their names on the paper.
• • •
Missing some Tweet in this thread? You can try to
force a refresh











