How effective are vaccines against Omicron?
Today 3 studies were posted of data on immune escape measured by reductions in "antibody neutralization titers".
We can use these to estimate VE, WITH SOME ASSUMPTIONS.
Thread based on paper w @billy_gardner_ that we'll post tomorrow
Today 3 studies were posted of data on immune escape measured by reductions in "antibody neutralization titers".
We can use these to estimate VE, WITH SOME ASSUMPTIONS.
Thread based on paper w @billy_gardner_ that we'll post tomorrow
We've known since the discovery of Omicron's growth & posting of it's sequence that it has many mutations in its spike protein, & many of these affect binding of our antibodies. @jbloom_lab estimated that these would reduce binding of antibodies 20-60 fold:
https://twitter.com/jbloom_lab/status/1468001874989121542
We measure "neutralizing antibody titers" by determining how much we can dilute a person's sera (blood) & have it still neutralize the virus & stop it from growing in cell culture. Papers often use 50% reduction in "plaques" or "foci" as a cutoff so you'll see FRNT50 as response.
We can compare neutralizing antibody titers for two virus variants & calculate amount that a virus escapes neutralization by calculating the ratio of neutralizing antibody titers for the two variants, and express this result as an X-fold reduction in neutralizing antibody titers.
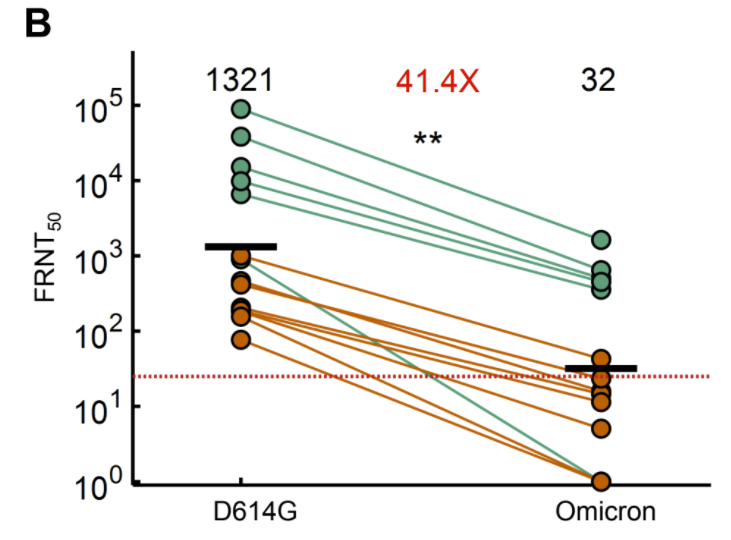
Today we got 1st actual data @sigallab on extent of neutralizing antibody escape. Live virus assay (gold standard) w/ 14 samples from 12 people suggested 41.4-fold reduction in titers, which is much higher than other virus variants.
ahri.org/wp-content/upl…

ahri.org/wp-content/upl…
https://twitter.com/sigallab/status/1468325159501287434
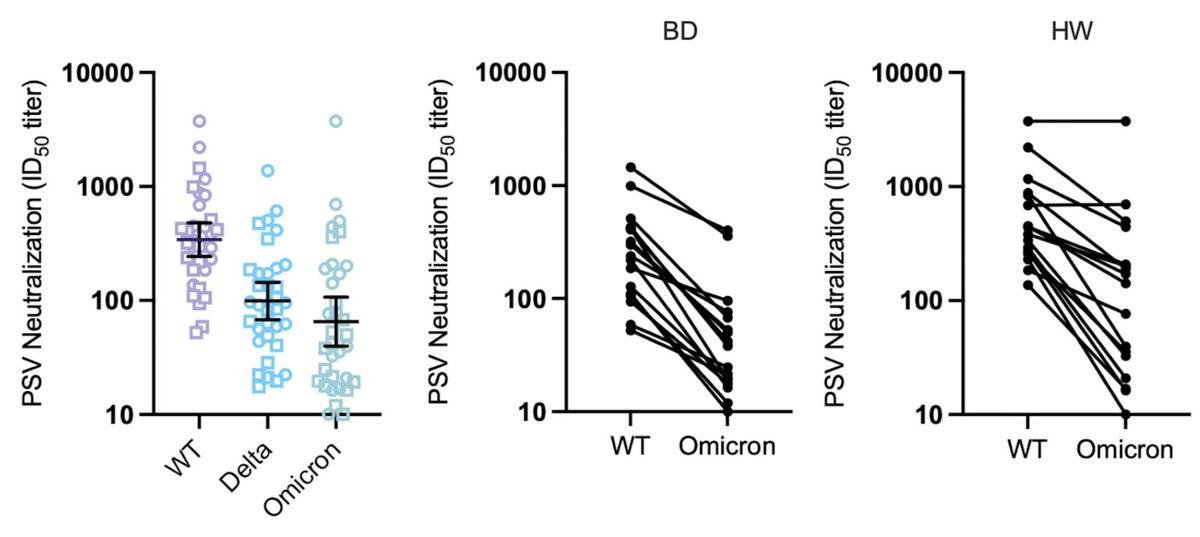
A 2nd study @BenjMurrell used a pseudovirus on blood from 14 people & estimated a smaller reduction - only 7-fold.
But when tested on a panel of "standard" WHO samples, reduction was 40-fold:
https://twitter.com/BenjMurrell/status/1468341478363746310
But when tested on a panel of "standard" WHO samples, reduction was 40-fold:
https://twitter.com/BenjMurrell/status/1468341501130428430
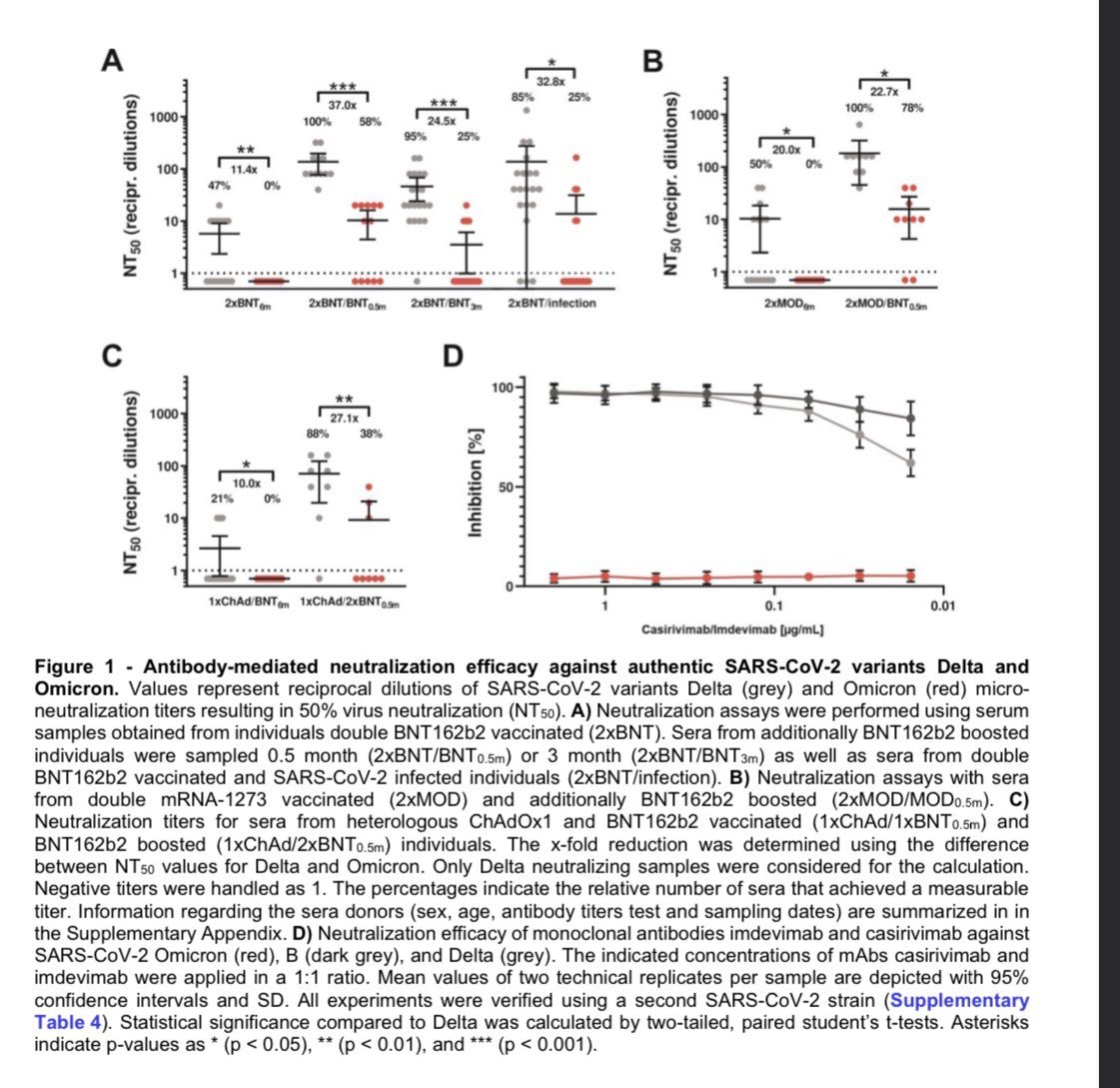
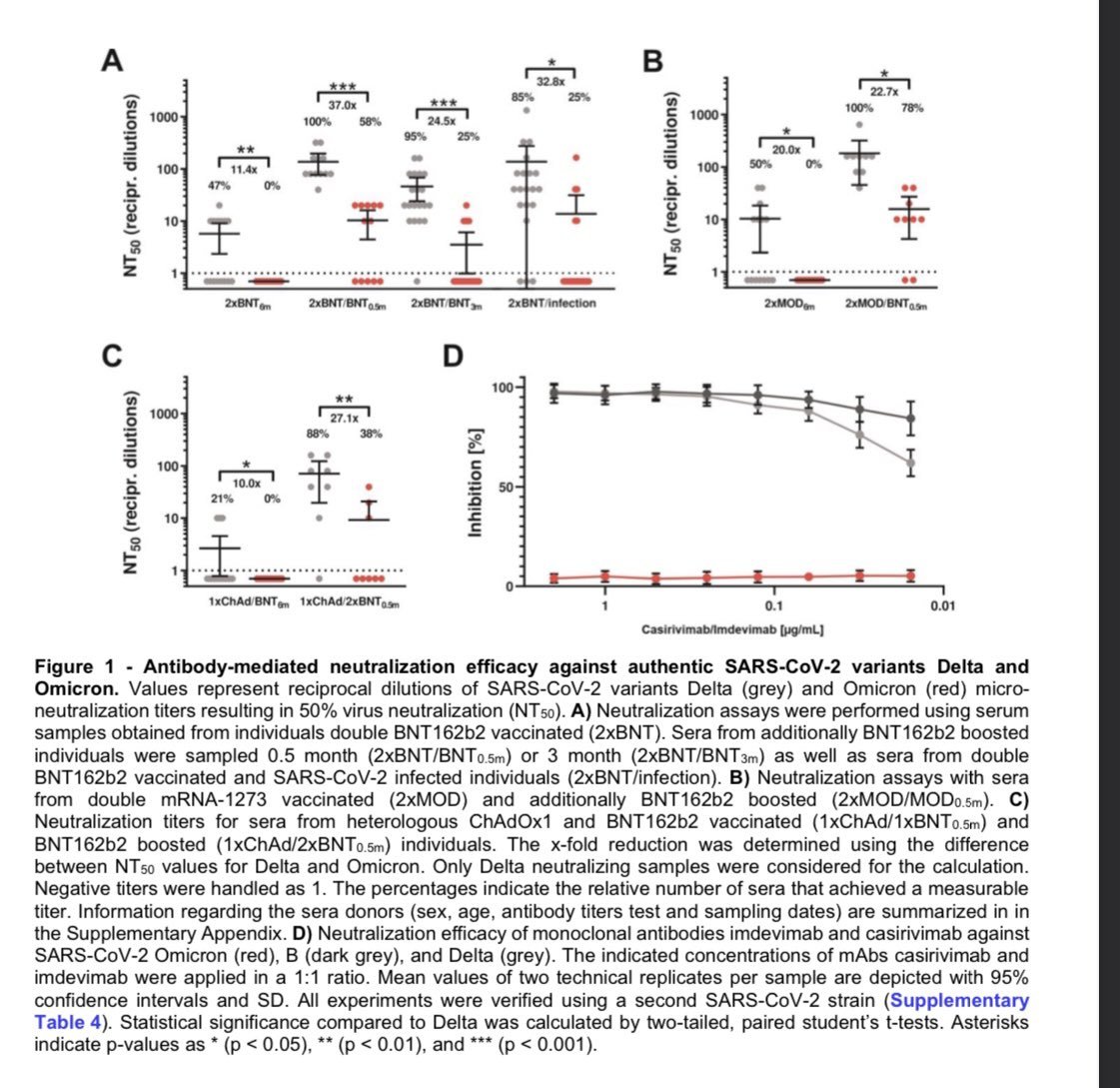
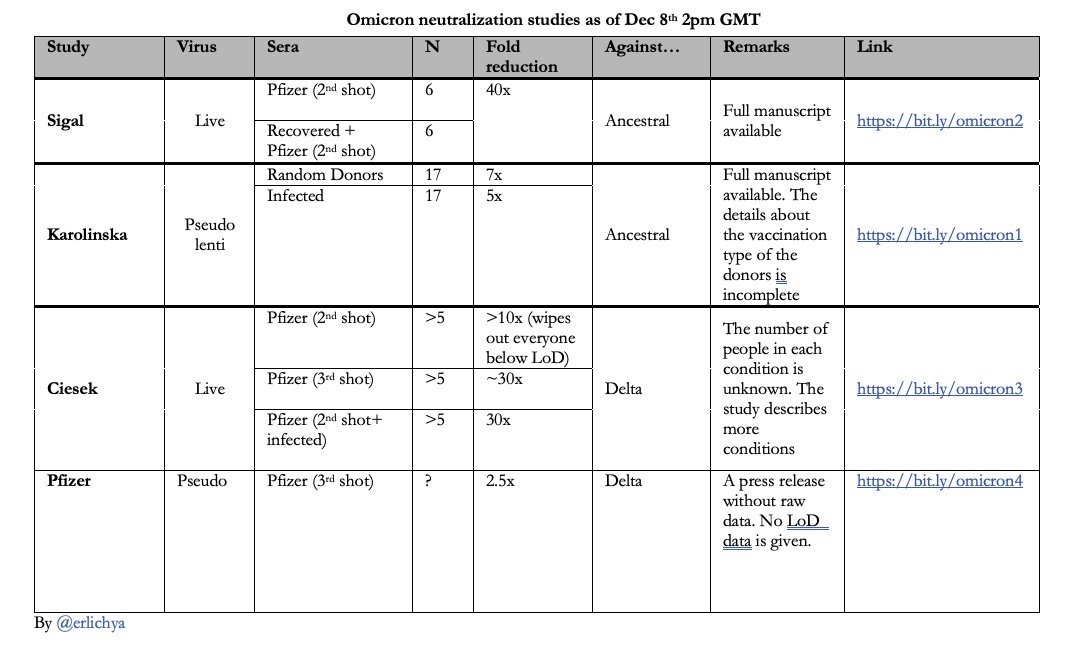
A 3rd study examined several vaccines & boosters & found 11-37 fold reductions
https://twitter.com/CiesekSandra/status/1468465347519041539
Several threads discuss these results in general:
But none estimate changes in VE from these results.
https://twitter.com/florian_krammer/status/1468397677562011650
https://twitter.com/profshanecrotty/status/1468390479280574472
https://twitter.com/biosbenk/status/1468379653735862277
But none estimate changes in VE from these results.
How much should we trust these initial results? Both studies above are relatively small.
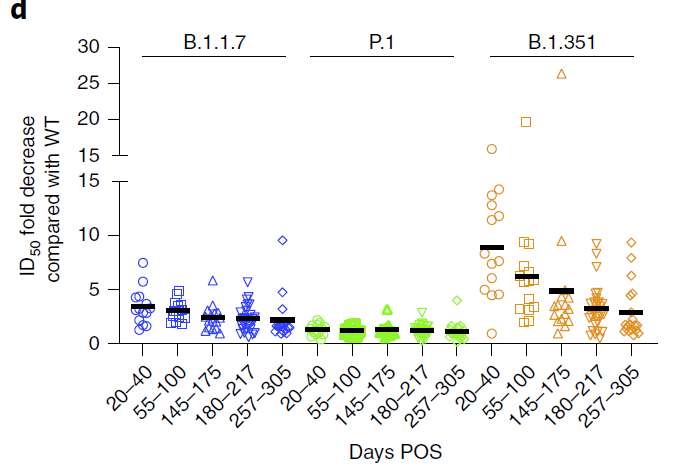
We (@billy_gardner_ & I) gathered data on relative reductions in neutralization titers from studies that compared at least 3 variants.
We (@billy_gardner_ & I) gathered data on relative reductions in neutralization titers from studies that compared at least 3 variants.
We found that measurements are moderately consistent in terms of relative differences w/in a study (lines in fig are parallel), but there are huge diffs b/w studies (methods, samples, etc.), so need to have all the variants you want to compare in 1 study.
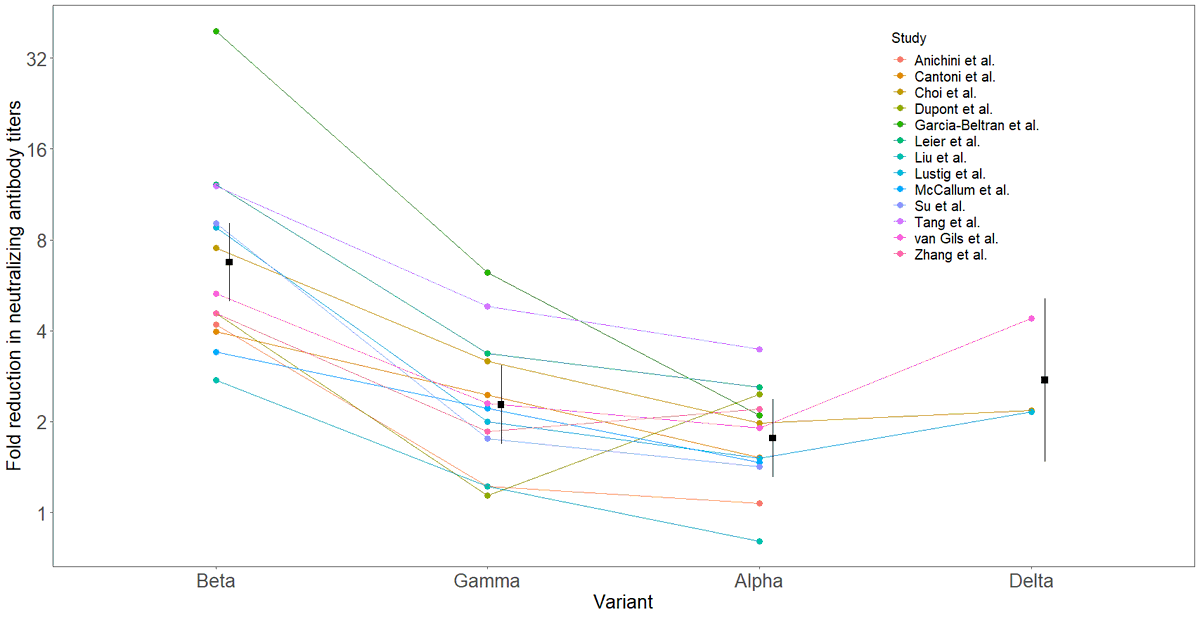
Studies above suggest a 7 - 41 fold difference, with weight leaning towards the upper end (20-40-fold reduction).
What does this mean in terms of vaccine effectiveness?
It does NOT mean a 20-40-fold reduction in VE. But...
What does this mean in terms of vaccine effectiveness?
It does NOT mean a 20-40-fold reduction in VE. But...
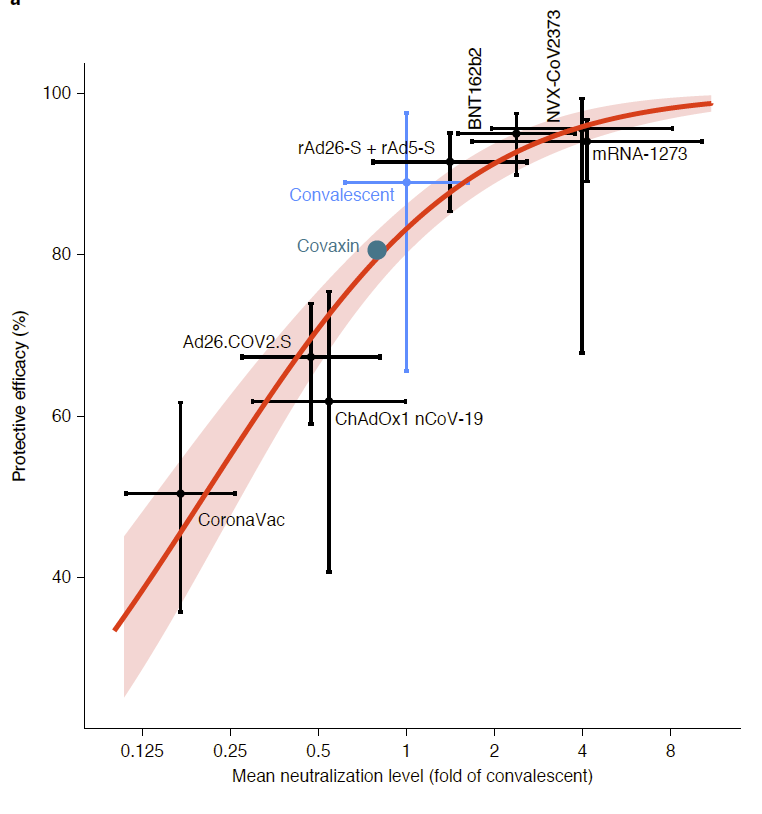
We can estimate the reduction using data on VE for a vaccine & neutralizing antibody titers. Two papers that did this are:
medrxiv.org/content/10.110…
nature.com/articles/s4159…
However - these studies compared VE across vaccines, NOT across virus variants. Can we do that directly?
medrxiv.org/content/10.110…
nature.com/articles/s4159…
However - these studies compared VE across vaccines, NOT across virus variants. Can we do that directly?
We used VE data from @alison_l_hill
medrxiv.org/content/10.110…
for specific vaccines & variants & paired them w/ neutralizing antibody titers for vaccines & variants to estimate VEs for symptomatic disease, doc infection & hospitalization.
medrxiv.org/content/10.110…
for specific vaccines & variants & paired them w/ neutralizing antibody titers for vaccines & variants to estimate VEs for symptomatic disease, doc infection & hospitalization.
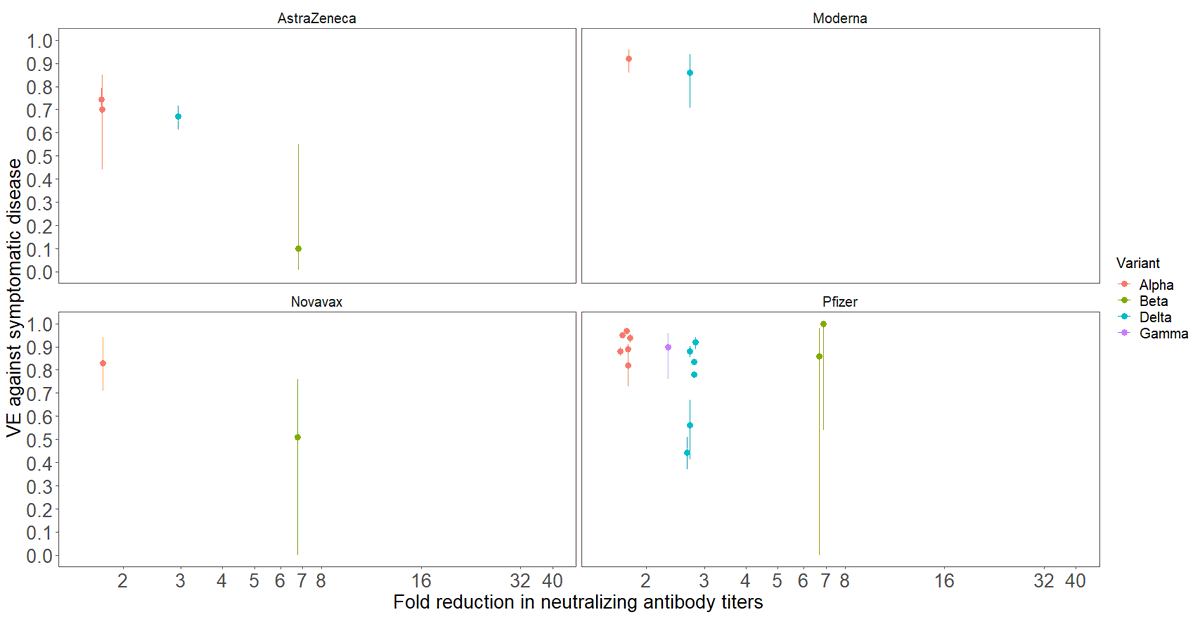
Here are VE for SYMPTOMATIC DISEASE & antibody neutralization fold-reductions for 4 vaccines & 4 variants. We could fit models to these data but notice empty space on graphs for >7-fold reductions - there are NO DATA. Thus we can't reliably estimate Omicron VE from these data.
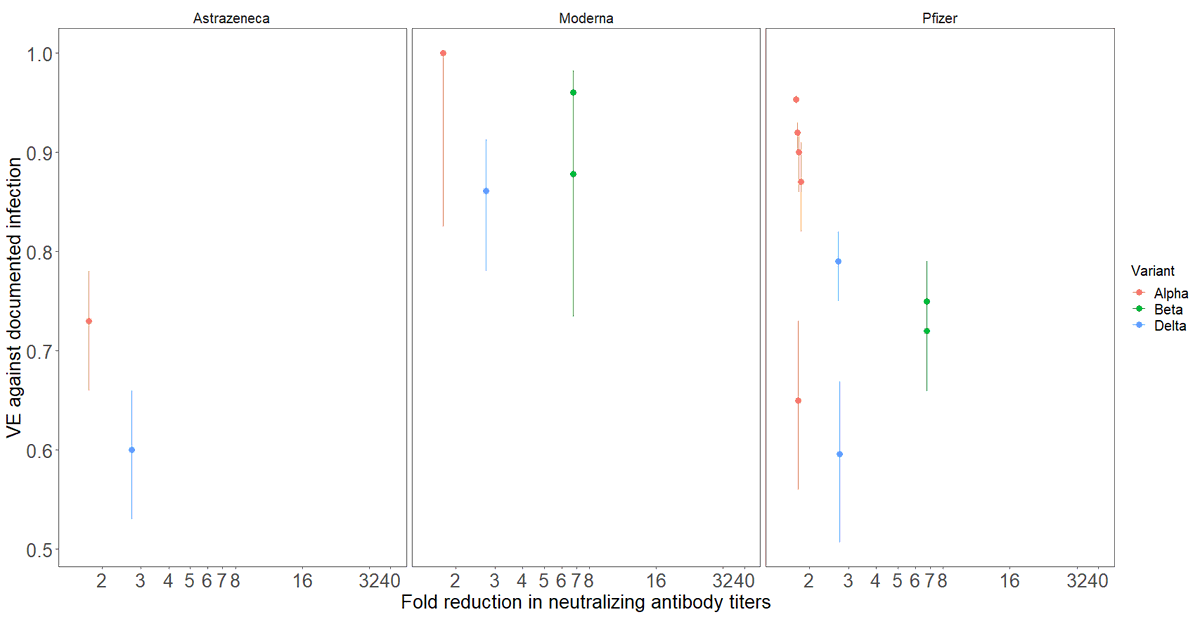
Here are VE for DOCUMENTED INFECTION (symptomatic + some unknown fraction of asymptomatic infections) vs. antibody neutralization fold-reduction. Again, no data w/ >7-fold reductions so no good estimates of VE for Omicron here.
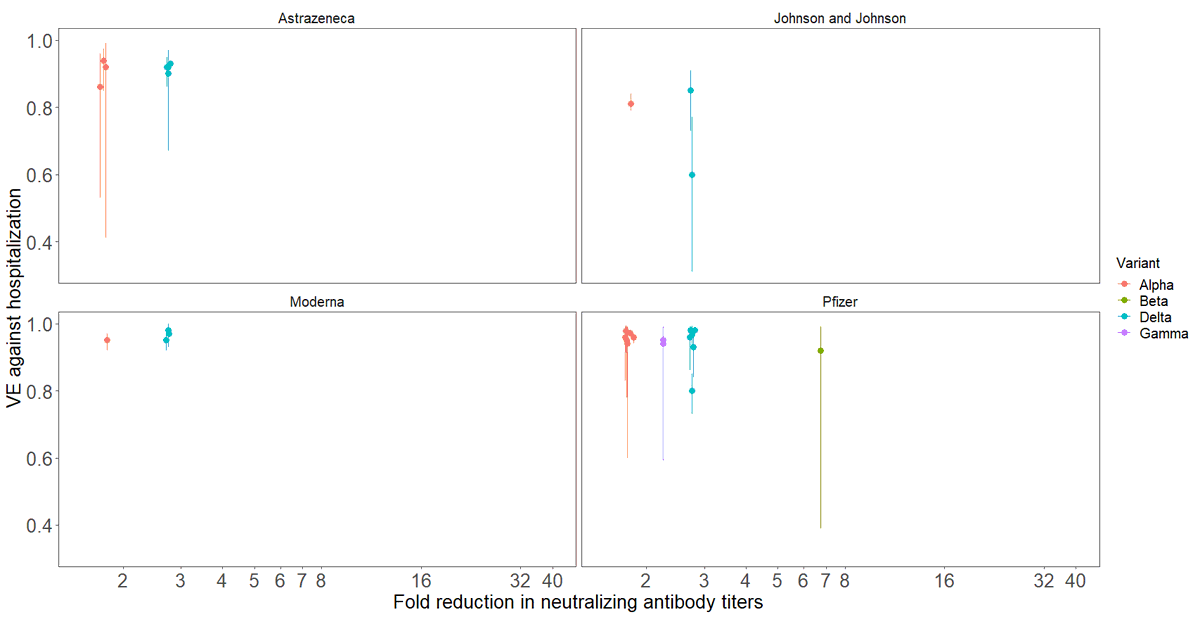
Finally, here is VE data for HOSPITALIZATION vs. antibody neutralization fold-reduction. Higher than last two endpoints (yay!) but again, no data w/ >7-fold reductions so we can't estimate VE for Omicron from these data.
(ps: Beta VE is highly uncertain for all endpoints)
(ps: Beta VE is highly uncertain for all endpoints)
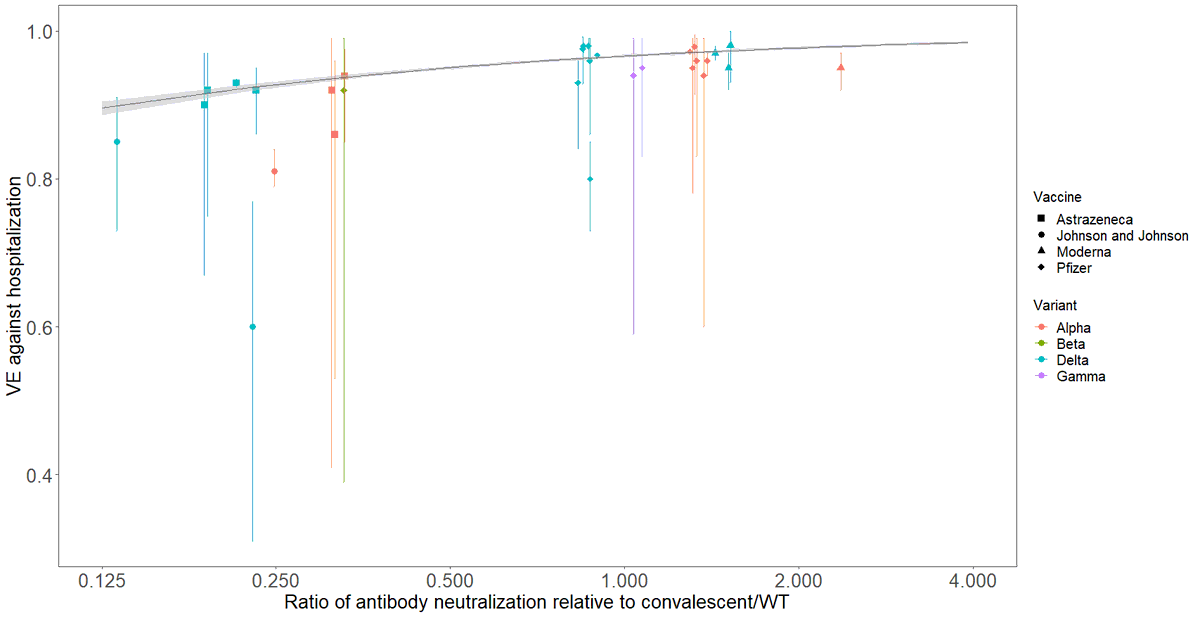
So what can we do? If we are willing to make a BIG ASSUMPTION that differences in neutralizing antibody titers ACROSS VACCINES & VARIANTS are valid for comparisons ACROSS VARIANTS, then we can do it b/c we have a much higher range of neutralizing antibody titers across vaccines.
Here are VE for HOSPITALIZATION vs antibody titers relative to original variant (WT) w/ all data from 4 vaccines & 4 variants on same graph; data spans 13.7-fold antibody titer range; predicted VE 89.6% (88.6-90.4) to 98.4% (98.2-98.7).
VE for HOSPITALIZATION is very robust!
VE for HOSPITALIZATION is very robust!
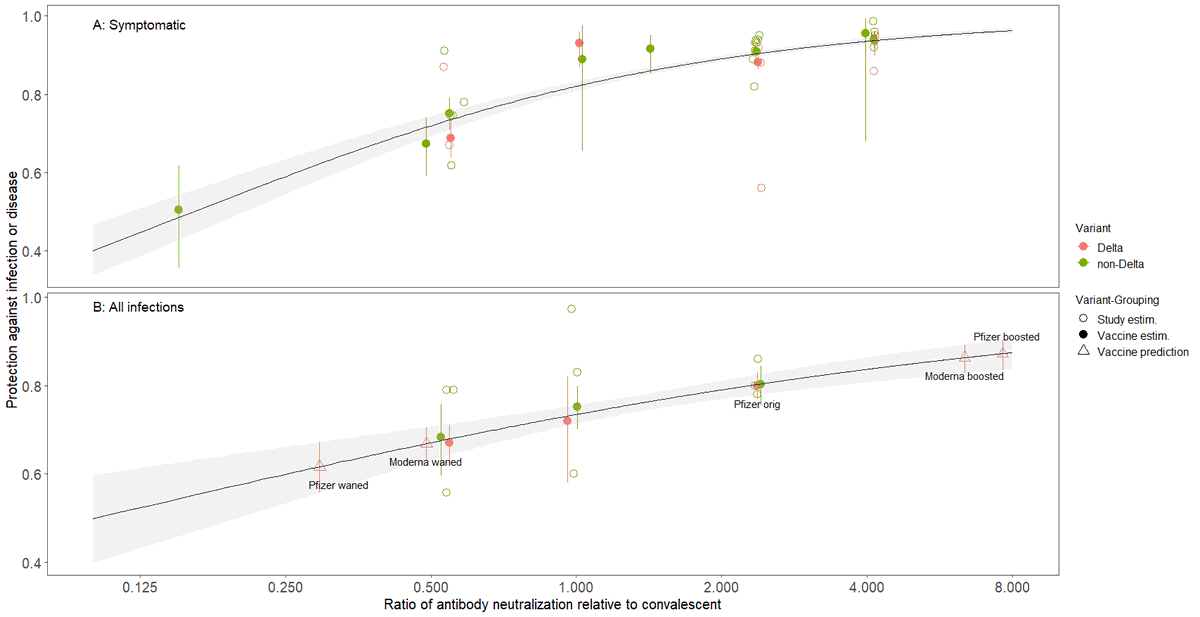
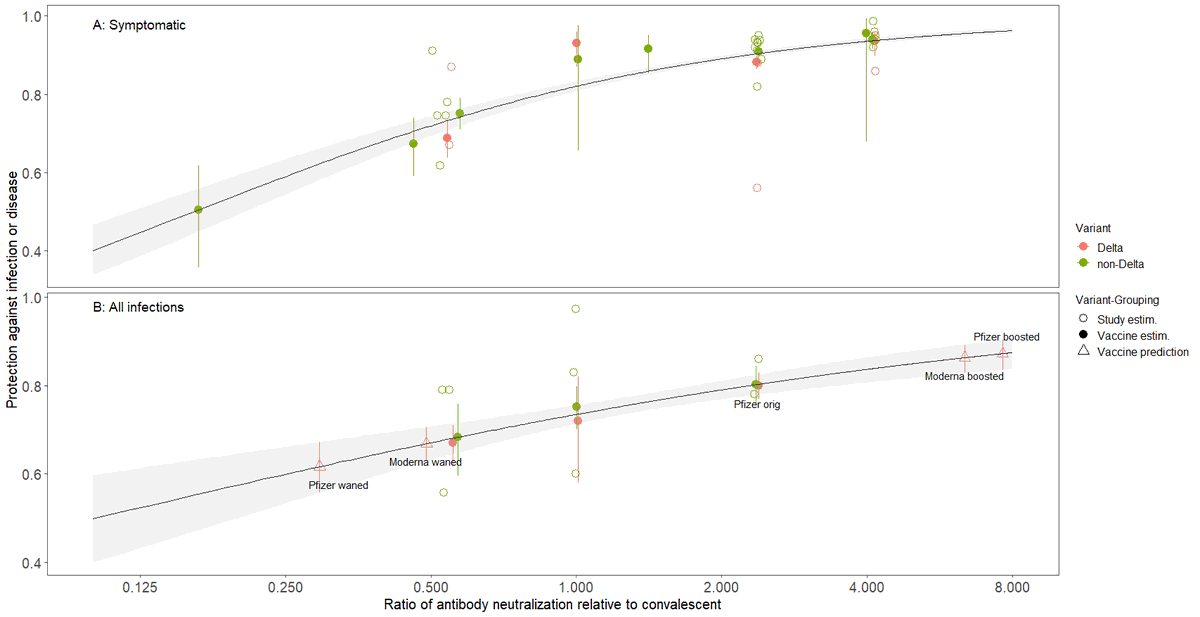
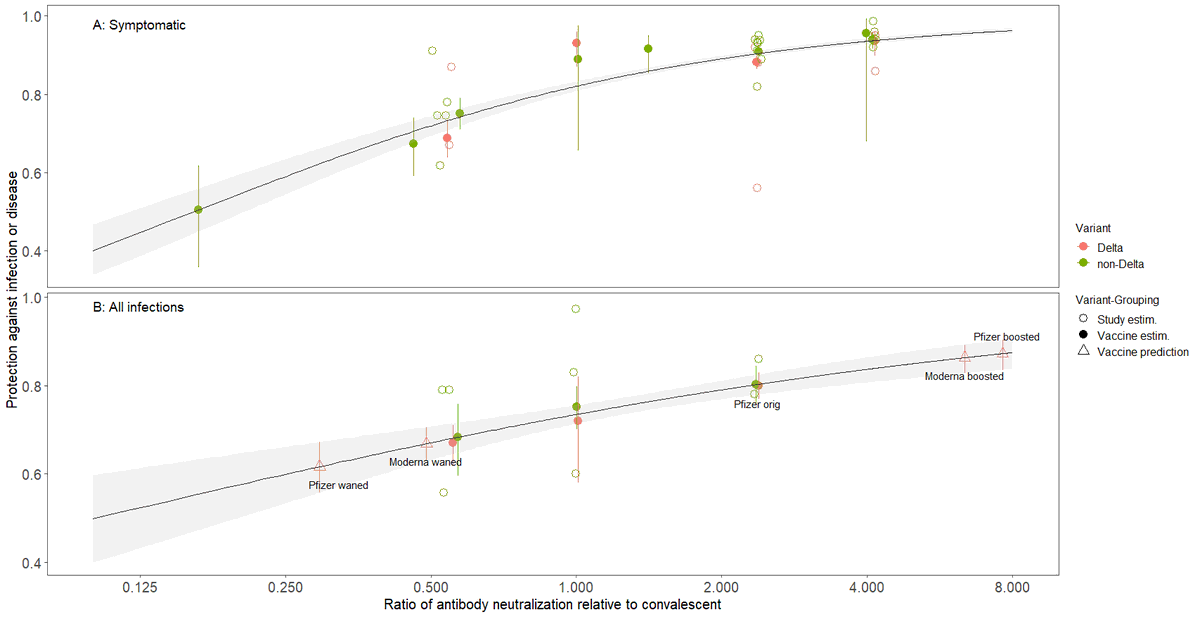
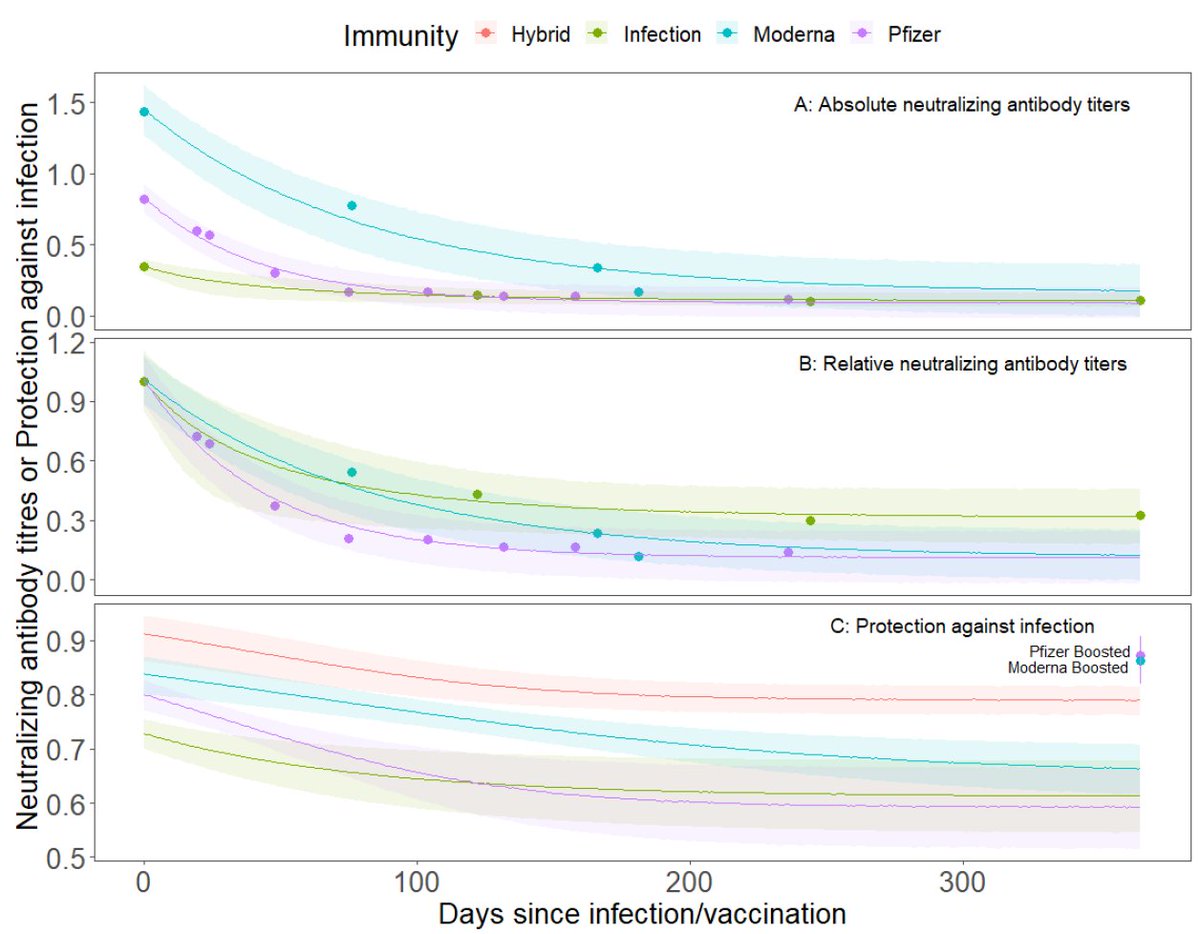
For symptomatic disease & ALL infections we can use relationships in our recent paper (updated fig below)
medrxiv.org/content/10.110…
These data span 45-fold range of neutralizing antibody ratios which ~=Omicron-fold reduction. So what can we say?
medrxiv.org/content/10.110…
These data span 45-fold range of neutralizing antibody ratios which ~=Omicron-fold reduction. So what can we say?
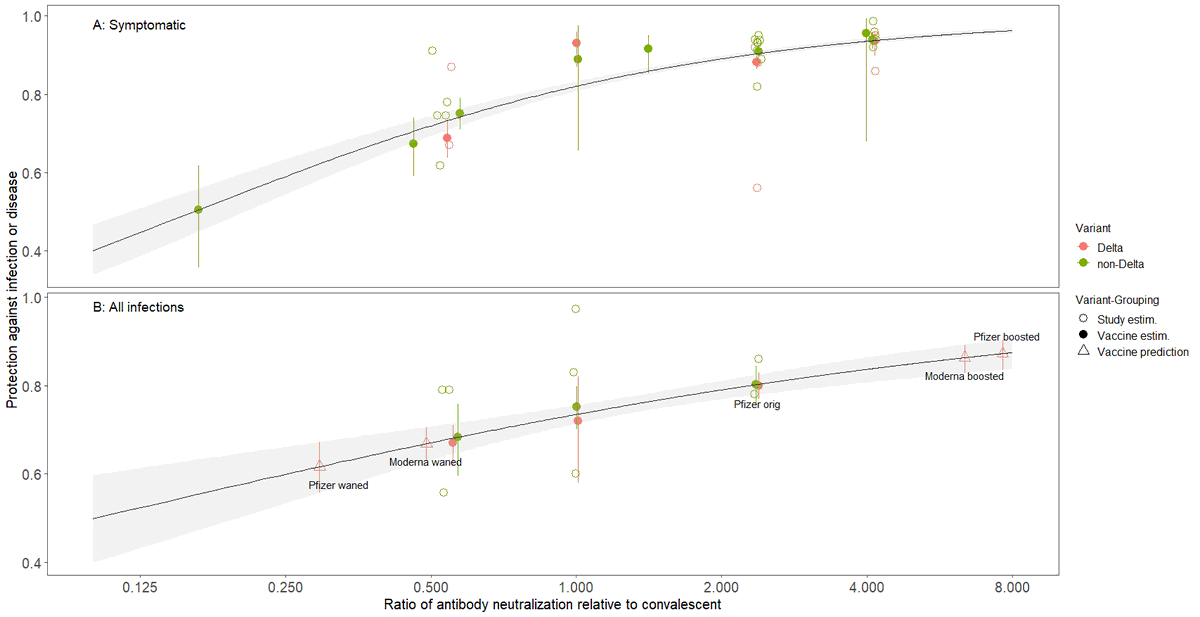
A fresh Moderna VE (i.e. 1-2 weeks post dose 2) for SYMPTOMATIC DISEASE was ~95% for original WT virus. w/ Omicron, assuming ~40 fold reduction, VE ~52% (35-60%), close to China's Coronavac vaccine.
Similarly, fresh Pfizer WT VE ~93% w/ Omicron: EXTRAPOLATION: 30% (24-37).
Similarly, fresh Pfizer WT VE ~93% w/ Omicron: EXTRAPOLATION: 30% (24-37).
What can we do to counter Omicron immune evasion? Get a booster, especially if 3-6 mo from vaccination!
In same paper medrxiv.org/content/10.110…
we show 3rd dose Pfizer boosts waned Ab 26x! 3rd Moderna boosts waned Ab 13x, but starts higher, so ~same! See panel B, red triangles.
In same paper medrxiv.org/content/10.110…
we show 3rd dose Pfizer boosts waned Ab 26x! 3rd Moderna boosts waned Ab 13x, but starts higher, so ~same! See panel B, red triangles.
Summary
Omicron's 30-40-fold reduction in neut. antibody titers will lead to ESTIMATED:
~10-14% reduction in VE HOSPITALIZATION
~40-60% reduction in SYMPTOMATIC INFECTION
Both of these can be mostly mitigated by 3rd dose booster.
Omicron's 30-40-fold reduction in neut. antibody titers will lead to ESTIMATED:
~10-14% reduction in VE HOSPITALIZATION
~40-60% reduction in SYMPTOMATIC INFECTION
Both of these can be mostly mitigated by 3rd dose booster.
Biggest Caveats:
-Indirect approach using antibody titers as correlate of VE
-Variation among vaccines can approximate variation among variants
-40-fold reduction sometimes required extrapolation, which is always dangerous
-Indirect approach using antibody titers as correlate of VE
-Variation among vaccines can approximate variation among variants
-40-fold reduction sometimes required extrapolation, which is always dangerous
I'd welcome comments, criticism, corrections.
@florian_krammer @nataliexdean @PeterHotez @JamesWard73 @profshanecrotty @mishkendall
@mlipsitch @michaelmina_lab @EricTopol @chrischirp
@florian_krammer @nataliexdean @PeterHotez @JamesWard73 @profshanecrotty @mishkendall
@mlipsitch @michaelmina_lab @EricTopol @chrischirp
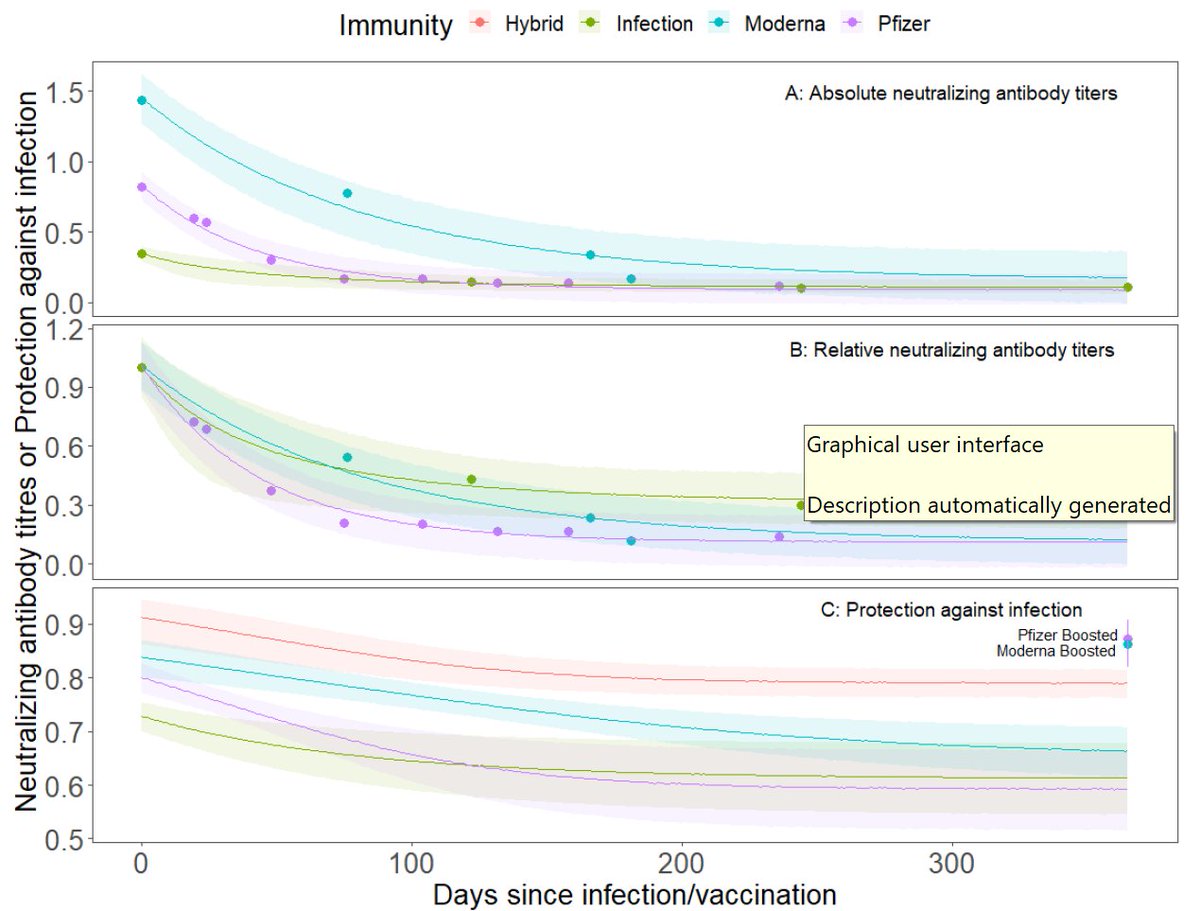
Clarification 1: impact of 3rd doses on antibody titers are relative to waned titers. So:
Waned Pfizer Ab + 3rd dose + Omicron ~= waned Pfizer Ab = ~60% vs all infections.
So very important to boost, but doesn't fully restore Ab to fresh 2d levels.
Waned Pfizer Ab + 3rd dose + Omicron ~= waned Pfizer Ab = ~60% vs all infections.
So very important to boost, but doesn't fully restore Ab to fresh 2d levels.
This is consistent w/ paper above (
https://twitter.com/CiesekSandra/status/1468465347519041539) showing *some* samples w/ booster didn't reach neut threshold. Note also that some boosted people were 3mo post 3rd dose.
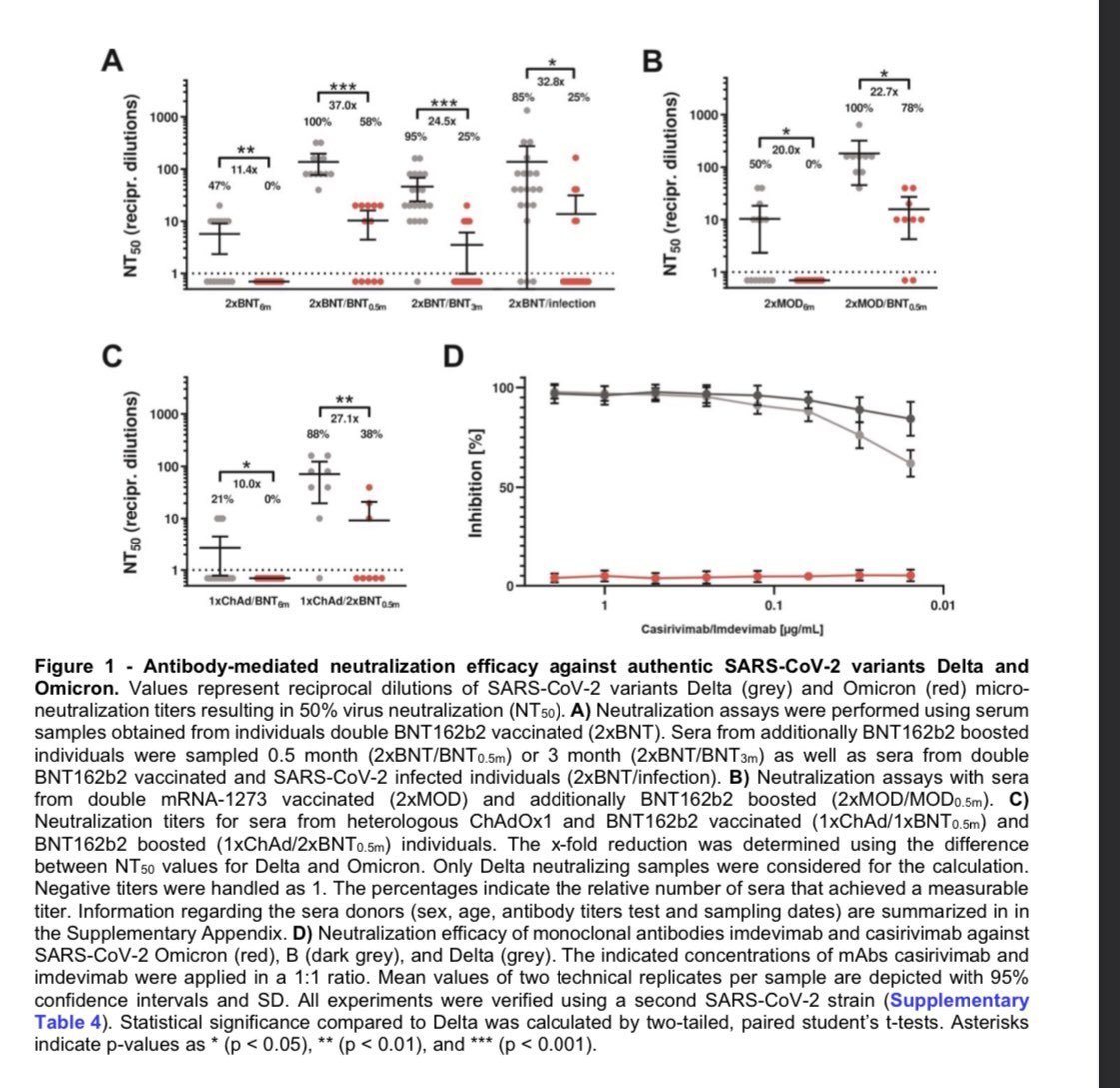
Clarification 2: Reductions in study just mentioned (
https://twitter.com/CiesekSandra/status/1468465347519041539) are RELATIVE TO DELTA. Our comparison above
https://twitter.com/DiseaseEcology/status/1468520447507501058suggests that reduction relative to WT would each be 2.7x higher. 11-37 becomes 30-99 but wide CIs.
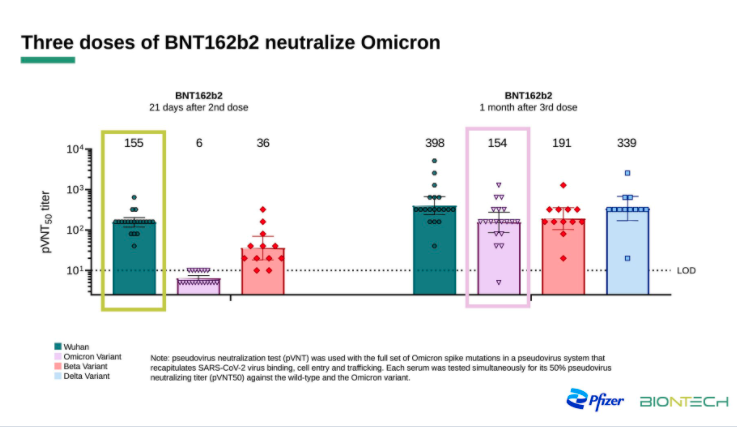
Add 1: Pfizer released 4th dataset on Omicron reductions & impacts of 3rd dose booster relative to 2dose (pseudovirus, n=19-20)
A 30x reduction for 2nd dose sera but only 2.6x for 3rd dose sera. Confusing right? Ratios also smaller for other viruses.
https://twitter.com/whippletom/status/1468582973775699981
A 30x reduction for 2nd dose sera but only 2.6x for 3rd dose sera. Confusing right? Ratios also smaller for other viruses.
This difference *could* be due to antibody maturation. It's been longer since vaccination for 3rd dose people & over time antibodies become more robust to mutations:
doi.org/10.1038/s41564…
It could also be due to variation among individuals incl. exposure b/w 2nd & 3rd doses.
doi.org/10.1038/s41564…
It could also be due to variation among individuals incl. exposure b/w 2nd & 3rd doses.
Looking forward to additional datasets to sort out differences among results in reductions in antibody titers & first direct VE estimates. Rapid Omicron spread already documented in Europe means VE estimates could come soon.
Correction: In Summary I left out VE. It should read:
Summary
Omicron's 30-40-fold reduction in neut. antibody titers will lead to ESTIMATED:
~10-14% reduction in VE HOSPITALIZATION
~40-60% reduction in VE SYMPTOMATIC INFECTION
Both of these can be partly mitigated by 3rd doses.
Summary
Omicron's 30-40-fold reduction in neut. antibody titers will lead to ESTIMATED:
~10-14% reduction in VE HOSPITALIZATION
~40-60% reduction in VE SYMPTOMATIC INFECTION
Both of these can be partly mitigated by 3rd doses.
Add: To folks wanting to calculate a waned VE, I purposely didn't report VE for waned mRNA vaccination w/ Omicron b/c that would be 9-fold x 40-fold = 360-fold reduction & that's way outside data. Suffice to say that VE for both Hospitalization & Symp disease would be quite low.
Add:
Table of 4 Ab results (lt fig):
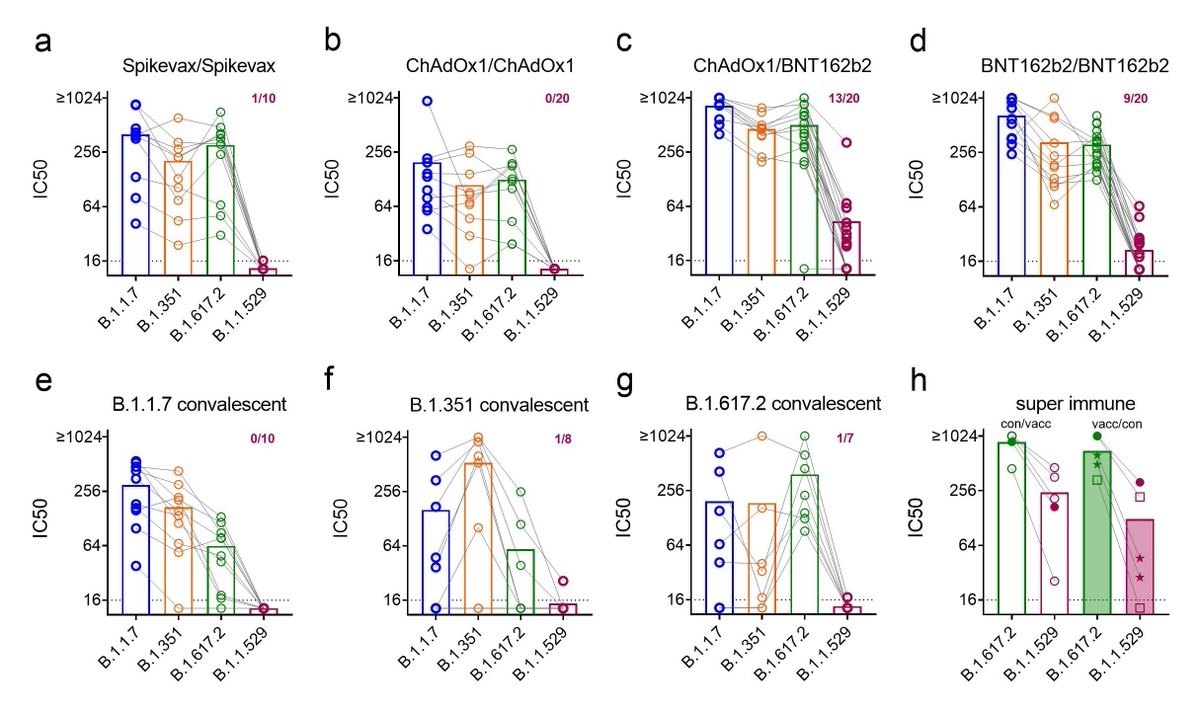
& 5th, live virus, (rt bot):
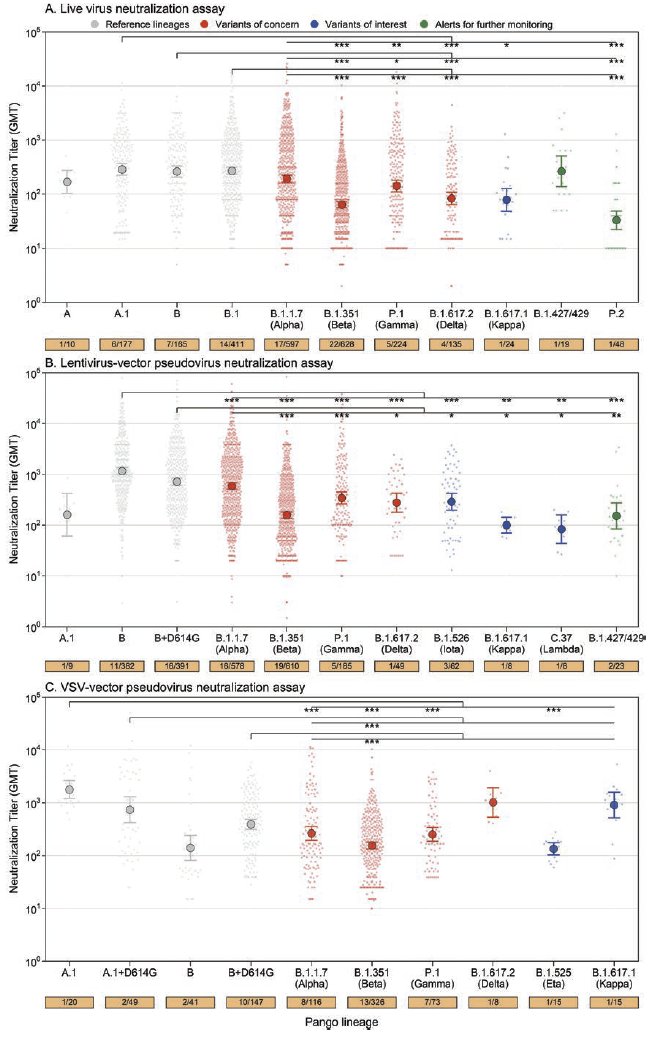
So far, live virus assays show more reduction in neutralization titers which is not always the case (rt top fig- but unpaired comparison):doi.org/10.1093/cid/ci…
Table of 4 Ab results (lt fig):
https://twitter.com/erlichya/status/1468580675007795204
& 5th, live virus, (rt bot):
https://twitter.com/JanineKimpel/status/1468700628922904591
So far, live virus assays show more reduction in neutralization titers which is not always the case (rt top fig- but unpaired comparison):doi.org/10.1093/cid/ci…
Clarification: VE estimates above all assume no intrinsic difference in omicron in terms of disease severity or that any diffs fall along line of other variants used to estimate relationships (alpha, beta, gamma, Delta). If omicron is inherently more or less severe all bets off.
Paper has been submitted to medRxiv. Until it posts, it's available here:
drive.google.com/file/d/1_KMMZf…
Let me know if you have trouble access the file. Code & data link in paper.
drive.google.com/file/d/1_KMMZf…
Let me know if you have trouble access the file. Code & data link in paper.
• • •
Missing some Tweet in this thread? You can try to
force a refresh