
An important study just posted from @BalazsLab
Findings are good for Pfizerites and Modernans but sobering for #JnJers
#JnJers even after boosting have lower neutralizing antibodies against Delta and Omicron vs 3x Pfizer
I'll discuss implications
🧵
Findings are good for Pfizerites and Modernans but sobering for #JnJers
#JnJers even after boosting have lower neutralizing antibodies against Delta and Omicron vs 3x Pfizer
I'll discuss implications
🧵
https://twitter.com/BalazsLab/status/1470727015896469505
Study design is excellent. Relevant vaccine statuses were tested in parallel: {Moderna, Pfizer, J&J} x {distant vax, recent vax, infection+vax, boosted vax}. Assay was pseudovirus neutralization. Color-coded images explain everything. 

Also there's a very informative diagram of what was actually done. A picture not just says 1000 words, but is so much easier to understand and prevents confusion about what reagents and procedures were used, so hoping this becomes more common in papers.

And now the good/bad news for RNA/J&J recipients. I'll put 3 images together so all the info is in one place.
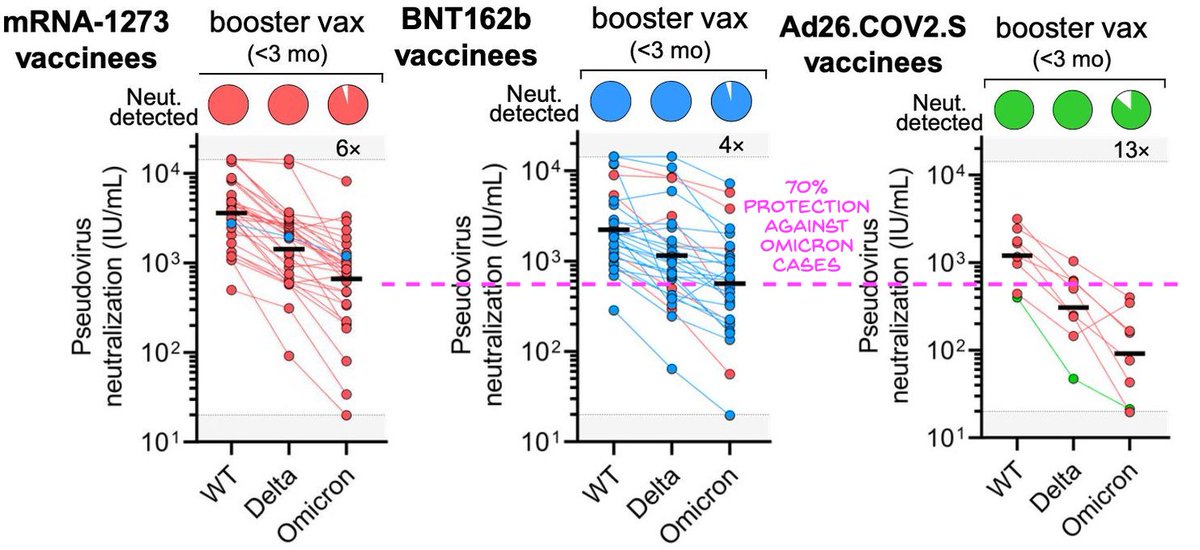
It's a lot of data but the patterns are clear. First, boosting works better than previous infection across all strains, WT, Delta, and Omicron (WT=wild-type=original)
It's a lot of data but the patterns are clear. First, boosting works better than previous infection across all strains, WT, Delta, and Omicron (WT=wild-type=original)



BTW the vax are color coded (very nice!), so in the booster column, you can tell which booster each person got! So one Modernan got a J&J booster, 3 Pfizerites got a Moderna boost, and all JnJers got Moderna except for one who got JnJ. It's great to see JnJers so well informed!

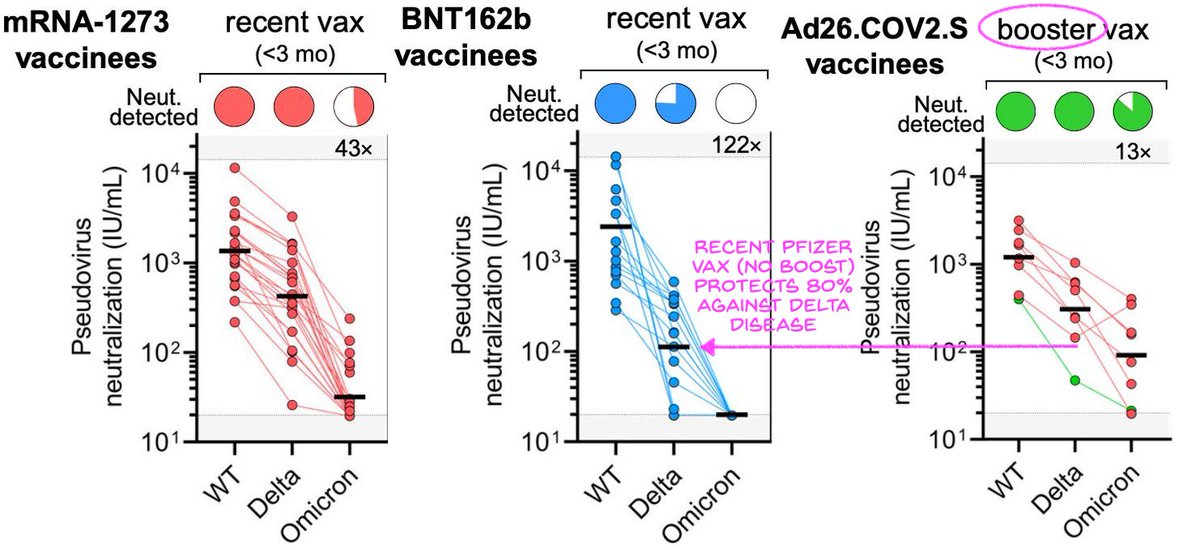
Now a very important result is that boosted vax is more effective on Delta and Omicron than unboosted recent vax. This is true even for Pfizer where WT neutralization is the same. As the vaccines are made to "WT" sequence, this means boosting is broadening the antibody response!

Another clear result is that J&J is inferior in all states. You can see across all states in tweet #4, or we can just look at the freshly vaccinated but unboosted state below. The freshly vaxxed state vs WT would reflect the conditions that earned J&J approval originally.

The inferiority of J&J confirms every other comparison study, such as the one below.
And we know peak J&J protection for WT was 66% vs >94% for RNA vax. For Delta, it's ~50% (Sisonke), vs 90/85% for Moderna/Pfizer. So nAb levels correlate with outcomes.
And we know peak J&J protection for WT was 66% vs >94% for RNA vax. For Delta, it's ~50% (Sisonke), vs 90/85% for Moderna/Pfizer. So nAb levels correlate with outcomes.
https://twitter.com/vivek_naranbhai/status/1470292266468130817
But the most concerning thing is this: J&J+booster doesn't work as well against new variants compared to Moderna+booster or Pfizer+booster.
You notice how J&J boosted is similar to Pfizer boosted for WT (especially if high Pfizer outliers removed), but much worse for variants.
You notice how J&J boosted is similar to Pfizer boosted for WT (especially if high Pfizer outliers removed), but much worse for variants.

Also because of the nice color-coding, we can see above that the JnJers who got Moderna boost (red) were better off than the one who chose a JnJ boost. Small n, but it's as we expect from the heterologous boost study. So can't claim the "wrong" booster.
https://twitter.com/michaelzlin/status/1466492316542111749
Pfizer says 3xPfizer gives 70% protection vs Omicron cases. We can then predict boosted Modernans will have the same protection, but boosted JnJers won't.

Conclusion: Modernans and Pfizerites are benefiting from a broadening of neutralizing antibody responses after boosting that helps neutralize variants.
JnJers don't have the same breadth in their nAbs after boosting. They will be less protected.
JnJers don't have the same breadth in their nAbs after boosting. They will be less protected.
What this suggests is that the initial humoral response elicited by J&J is materially narrower than those elicited by RNA vaccines. As a result the memory B cell expansion induced by boosters results in a broader set of nAbs in Modernans and Pfizerites than JnJers.
This also means the limited humoral response of the J&J vaccine, long waved aside by Ad proponents who claimed the Ad vaccines had better T cell responses, does indeed lead to a meaningful functional disadvantage.
Finally what can be done? I think it's pretty clear. JnJers need a RNA vax dose at some point to prime a wide memory B cell population, and then need to be boosted to get the broad antibody response to protect against Delta and Omicron.
JnJers who got boosted by Moderna or Pfizer have that RNA dose already. They would benefit greatly from another shot any time after 1 month (based on other studies, 3 months is probably ideal for max response). This "another" shot can be RNA (guaranteed) or could be J&J (below)
Essentially J&J is not a good way to start a vaccine series when we are faced with variants against which a broad antibody response is useful. Instead a J&J primary vaccine should be considered similar to a natural infection: not enough vs variants.
JnJers who haven't gotten a RNA booster should be told to get one 2 months after their last J&J, and then another booster 6 months later. They can benefit from the wider B cell repertoire. If they are in a vulnerable population, they absolutely will need it.
It would makes sense to deprecate J&J to the role of a booster to the RNA vaccines (where it seems to work well enough, see green dot below, and may give a broader CD8 T cell response).

Basically you need a RNA vaccine at some time to prime a wide B cell population for antibodies against variants. J&J does not substitute. If you don't do it earlier, you'll just have to do it later. I hope for the health of JnJers that @CDCgov and @CDCDirector will consider it.
@CDCgov @CDCDirector A couple of clarifications: As 2x RNA didn't produce nAbs vs variants (that's the recently vaxxed but unboosted case) but a 3rd shot of any sort did, it means 2x RNA may be needed to activate that broad memory B cell population. So for omicron JnJers may need 2x RNA in sequence.
Second, J&Jers boosted with Moderna should do fine against Delta. J&J + Moderna gives even more nAbs against Delta than 2x Pfizer unboosted (below), and that correlates with 80% VE against Delta disease. This is consistent with the previous prediction at
https://twitter.com/michaelzlin/status/1466488989003616257
So in a sense JJ+RNA booster gets to where 2xRNA was to begin with (pic1 below). But it is worse than 3xRNA for variants, esp Omicron (pic2 below). And with decay we expect some loss of protection to Delta in the upcoming months (if we go by 2xPfizer decay, maybe 50% VE at 6mo).

Made a mistake above regarding J&J as a booster. I misread a case of Moderna+Pfizer (blue dot) as Moderna+JJ (green dot). So this study doesn't say how well J&J works as a boost for RNA vax.
The earlier study says J&J is inferior to RNA in boosting nAbs
The earlier study says J&J is inferior to RNA in boosting nAbs
https://twitter.com/michaelzlin/status/1466488989003616257
Another way to explain the data is that 3 immunizations are needed for broad nAbs. Note the infection+2xRNA nAb levels are after 6mo decay; if the sera had been obtained soon after the last shot, those levels might be similar to recent 3xRNA.

Since 1xJJ is similar to infection by WT strain (ref below), then we expect that after a second RNA boost (i.e. JJ+RNA+RNA) then nAb levels may be like 3xRNA.
So this is even more reason to advocate for a 2nd boost.
nature.com/articles/s4159…
So this is even more reason to advocate for a 2nd boost.
nature.com/articles/s4159…
And if we now space the two RNA shots 2-6mo apart then one gets 2-4x higher nAbs than the original 3-4wk interval (sciencedirect.com/science/articl…). Note the most evasive Beta variant sees the biggest benefit, suggesting activation of a broader set of B cells with the longer interval.

Above I wrote 3mo as ideal interval in one tweet and 6-mo two tweets later. 3 or 6 mos between RNA shots 2 and 3 elicit similar peak nAbs, based on my skimming of the studies. So anything from 3 to 6 mos would work and timing could be based on when omicron protection needed.
In sum, 1x J&J is at most like 1 dose of RNA (seen as far back as phase1 antibody measurements). That's been reinforced by its use as a booster where it's worse than 1 dose of RNA.
But 1xJ&J and 2xRNA (but not 1xRNA) were designated as vaccinated. This has led to confusion since
But 1xJ&J and 2xRNA (but not 1xRNA) were designated as vaccinated. This has led to confusion since
CDC could clarify and rationalize guidance, significantly improving understanding and health, by shifting to a simple counting system.
"Make sure you get 3 shots, at most 1 J&J, and space them 2-6 months apart" is all they need to say
"Make sure you get 3 shots, at most 1 J&J, and space them 2-6 months apart" is all they need to say
And vulnerable 2xRNA-vaccinated can schedule that 3rd dose before 6mo by declaring themselves immunocompromised. This policy was from back when Pfizer+Moderna's studies found a need, while J&J didn't do studies although JJ was even less protective.
cdc.gov/coronavirus/20…
cdc.gov/coronavirus/20…
I get asked whether to get 100mcg Moderna (original dose), 50mcg Moderna (booster), or 30mcg Pfizer (original and booster). As mentioned below, you'd expect 100>50>30 in potency since RNA is RNA. But some people asked if diffs in the lipid carriers matter.
https://twitter.com/michaelzlin/status/1466492316542111749
Moderna found 100mcg and 50mcg Moderna 3rd doses raise nAb levels against Omicron by 87x and 37x respectively. Pfizer found its 30mcg booster raises nAbs by 25x.
The Mod and Pfizer results are in different studies but so far it seems 100>50>30 indeed.
telegraph.co.uk/global-health/…
The Mod and Pfizer results are in different studies but so far it seems 100>50>30 indeed.
telegraph.co.uk/global-health/…
Many are wondering if they can boost earlier than 6mo. The NIH heterologous boost study used 3mo after initial series (1xJJ or 2xRNA). Pfizer tested 8mo after 2xRNA. Results were similar, suggesting 3-8mo all ok. CDC guided 6mo because immunity waned to <50% VE against Delta then
And now Israel is allowing boosters 3mo after the previous shot. This will allow those 3mo out from last shot to get boosted ahead of winter, whereas earlier you had to wait for 6mos.
usnews.com/news/health-ne…
usnews.com/news/health-ne…
• • •
Missing some Tweet in this thread? You can try to
force a refresh









