
Finally, what we've been waiting for: age-controlled data on Omicron severity, courtesy SA health ministry.
Across all ages, deaths among hospitalized pts are 2/3 lower in Omicron wave.
If more mild cases are admitted, this # goes down, but doesn't seem likely that's the reason
Across all ages, deaths among hospitalized pts are 2/3 lower in Omicron wave.
If more mild cases are admitted, this # goes down, but doesn't seem likely that's the reason

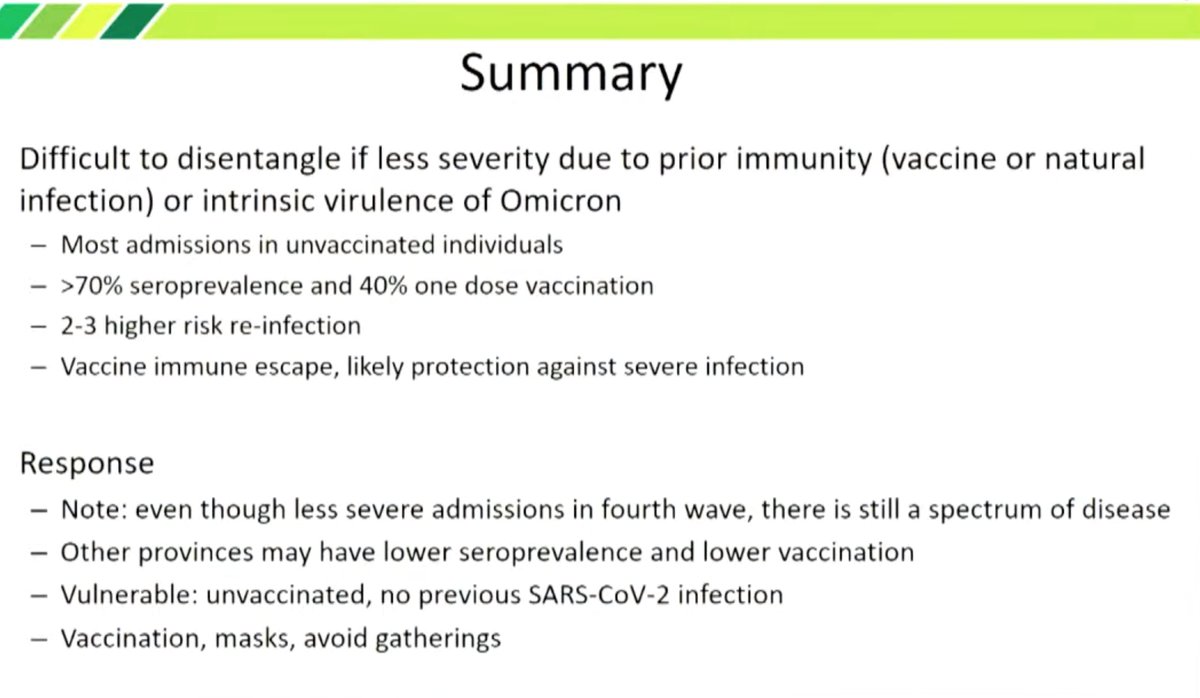
@b_chinnian5 Importantly, they said the vast majority of hospitalized cases were unvaccinated. But SA has a high rate of seroprevalance, >70% per some studies. So worst-case interpretation here is everyone hospitalized was either vaccinated or unvaccinated but previously infected.
Since most hospitalizations are unvaccinated, then the relative risk of death for vaccinated is already several times lower than for unvaccinated but maybe previously infected. Overall both groups have an average fatality rate of ~1/3 of previous waves.
So worst case:
• Unvaxxed infected IFR ~0.3% (assuming 1% for unvaxxed uninfected in previous waves, and similar hospitalization rate for Omicron)
• Vaxxed IFR several times lower (depends on ratio of unvaxxed to vaxxed in the hospitalized group)
• Unvaxxed infected IFR ~0.3% (assuming 1% for unvaxxed uninfected in previous waves, and similar hospitalization rate for Omicron)
• Vaxxed IFR several times lower (depends on ratio of unvaxxed to vaxxed in the hospitalized group)
Best-case scenario: Most hospitalized patients were immune-naive because those who got hospitalized tended to be those without prior immunity, in which case the lower death rate means Omicron is inherently less deadly as well.
Since it is true that many cases are being discovered in admits for other reasons, I should modify the statement in the first tweet that it's unlikely because of a larger denominator. It could be.
I think it's really the fact we're now weeks from the upswing and we haven't seen the same hosp rate as earlier waves at an equivalent time that suggests this wave is milder. Now this could be because >70% have some immunity, which would be similar to the US situation.
The data today are reassuring nevertheless, because it shows lower deaths across ages. Whether that's due inherently lower virulence or widespread immunity now, it means we can adjust SA's IFR by age alone, and don't need to worry that Omicron has a different age-severity fxn.
However we must remember omicron severity is still worse with age and other conditions, so countries with older age distributions or more unhealthy people will have higher overall deaths per capita from Omicron than SA even if they have similar % immunity.
Overview of cases vs hospitalizations. Always the caveat of now knowing how much underreporting of cases is occurring relatively between waves.
https://twitter.com/hivepi/status/1471721404747948039
And maybe the shortest wave so far
https://twitter.com/tomtom_m/status/1471723711287996416
@johnklopfer points out they are counting all cases in the hospital regardless of when the cases were detected. As case #'s are going up, many recent cases will be counted before they have the time to lead to severe disease. This will lower the apparent hospitalization death rate
In addition, many are apparently detected as positive but were hospitalized for other reasons; so this also increases the denominator of "hospitalized COVID19 patients" (many are not there for COVID19)
However these data are useful in showing there isn't a different skew to death rates by age for Omicron vs earlier variants. This is important because SA *has* shown lower severe disease in this wave than previous waves, but we've been warned this could be an age-dependent effect

That is, SA is younger than other countries. So, if Omicron is only milder for younger people, then the ~50% reductions in hospitalizations seen this wave (and yes, accounting for delay) might not apply to other countries with older populations.
However the data in post 1 shows the same age distribution as in previous waves, suggesting Omicron is not selectively sparing younger people. So it's the historical hospitalization/rate data that implies lower severity, and the deaths by age data argues it's not age-specific.
Even better would be historical case, hosp, and death curves broken down by age so we can confirm this. Not sure if SA hospitals report hospitalizations by age.
Here's some data that suggests ~90% of hospitalized cases with COVID19 in Gauteng province were indeed admitted for COVID19, so the contribution of mild/asymptomatic incidental COVID19 diagnoses to the "hospitalized COVID19" population appears minor.
https://twitter.com/enjoyingthewind/status/1472329401585045518
It's a bit odd when people warn SA is not representative of Western countries due to high seroprevalence >70%. Most Western countries are at the same from vaccination >60% and prev infection >25%. No linkage gives sero+ >70%. If no vax linked to prev infection, then even higher.
As long-term followers know, I tend to be more pessimistic than authorities and to call for more stringent measures (masks, boosters). For example in June I insisted there would be a Delta wave although some famous tweeters had already concluded not
https://twitter.com/michaelzlin/status/1410474227967225857
With Omicron I feel like I'm going out on a limb in the other direction for the first time. This wave resulting in fewer deaths per case than earlier ones seems the most parsimonious prediction from findings so far.
It's also what we'd predict from our existing immunity levels and omicron evasiveness: when you have something that creates a high rate of breakthru cases but 80% of popn has some immunity, then you expect a low death/case ratio.
We are still seeing a bump in hospitalizations and waves for sure, but I predict their numbers will be significantly lower per case than earlier waves in the US and Europe, because there are much fewer immune-native to infect, and many more with immunity to get breakthroughs in
The point is, replying to warnings not to divide today's hosp # with today's case #: Yes, I am very aware, and this was an error others made in the past, so it's good we're learning. But my analysis here, as before, accounts for a 2-wk delay between cases and hospitalizations
We're also seeing a low hosp/case rate in Denmark even with the proper 2 week wait for hospitalizations after cases. They've had Omicron for a month now. 2 weeks ago there were 7000 daily new cases, and today 15 new hospitalizations
irishtimes.com/news/health/ea…
irishtimes.com/news/health/ea…
Now Gottlieb with a similar tweet on the curves.
https://twitter.com/ScottGottliebMD/status/1472664060445569026?t=H6CqCClpEReoNaFnZGt_oA&s=19
Very important study from SA comparing hospitalization rates in the current wave between omicron and non-omicron COVID19 cases. Omicron cases have 80% reduced hospitalization risk. It's controlled for time & demographics so suggests inherent lower severity
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
Since vast majority of cases now are Omicron, that 80% reduction in risk of hospitalization compared to non-Omicron (presumably Delta) would easily explain the >50% lower hospitalization/case ratios in the current wave compared to the Delta wave.
Incidentally they also find that once hospitalized, Omicron cases have similar outcomes as non-Omicron cases. They attribute this to prev immunity helping both types of cases to get the same outcomes, as these outcomes are less severe than previous waves for non-Omicron too
I spent 2020 debunking all these right-wing excuses for why COVID19 won't hit the US so badly because of different demographics habits diets genetics etc. Ironic now how people are grasping at similar straws to argue we have no evidence the Omicron wave will be less severe
• • •
Missing some Tweet in this thread? You can try to
force a refresh









