#JanuAirway Day 5. Airway Planning. Decision making is the true art of airway management, and something that we don’t really get taught! NAP4 @doctortimcook showed that poor judgement was implicated in many airway complications. Here’s a #OnePager covering the major themes. 1/16 



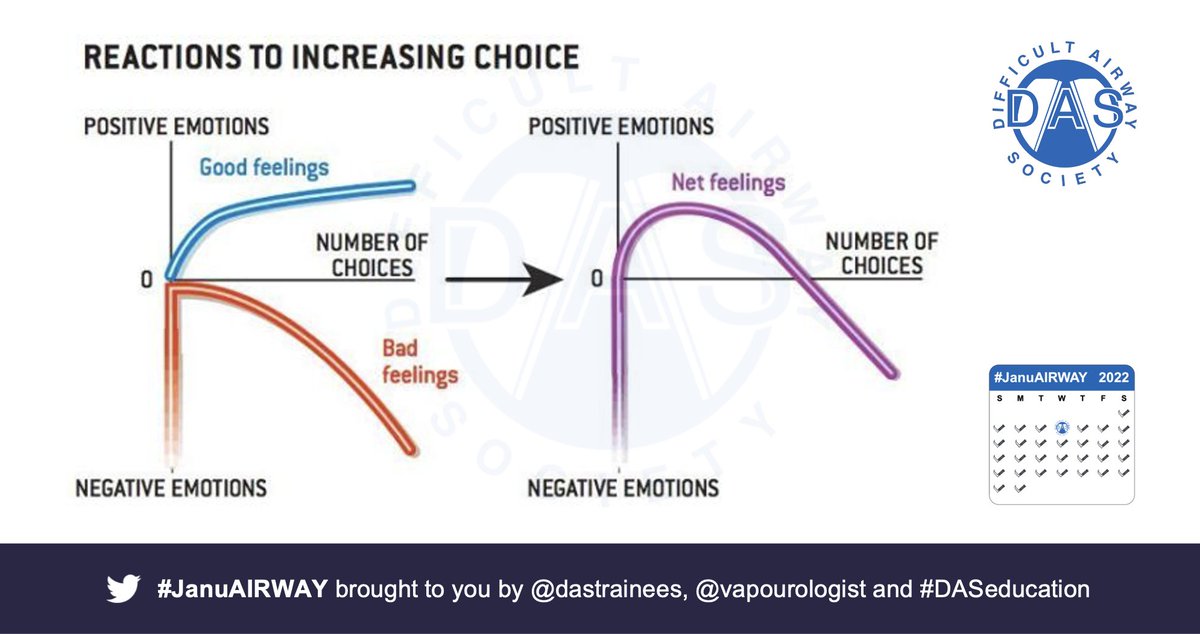
#JanuAirway Why is this an issue? Difficult airways = relatively rare & complications = rarer still. Low exposure --> high anxiety. Add in multiple options @AirwayMxAcademy & Bouwman suggest >1,000,000 combinations of options to oxygenate. More options = more anxiety 2/16
#JanuAirway
Cognitive load can lead to decision fatigue/increased bias/poor choices. Chew et al’s ncbi.nlm.nih.gov/pmc/articles/P… TWED metacognition checklist may help: -
Threat– define problem
Wrong- What if I’m wrong?
Evidence
Dispositional factors – environment/hunger/fatigue 3/16
Cognitive load can lead to decision fatigue/increased bias/poor choices. Chew et al’s ncbi.nlm.nih.gov/pmc/articles/P… TWED metacognition checklist may help: -
Threat– define problem
Wrong- What if I’m wrong?
Evidence
Dispositional factors – environment/hunger/fatigue 3/16
#JanuAirway The Elaine Bromiley & Gordon Ewing cases are essential reading – highlight competing problems with task fixation and failure to accept safe (but not necessarily desirably situations). Here are the key issues & a decision cycle as a way of combating both 4/16

#JanuAirway Situational awareness is key. Define your thinking zones & the kind of situation you are in. Try to limit your options, but think holistically about the whole airway – @vapourologist uses this 3 step approach with his ADEPT mnemonic 5/16



#JanuAirway You’re not alone in having airway skills – remember your surgical colleagues & involve them early. BUT remember not all surgeons are equal (same as anaesthetists!) – having subspecialty interests a rhinologist might not be comfortable doing FONA either! #FOAMed 6/16


#JanuAirway Putting it all together – consider an airway strategy sheet, like the this one – define problems / limits up front, involve ENT early, define plans ABC&D – consider all options, but decide on a few
#FOAMed 7/16
#FOAMed 7/16

Here are some papers / links that you might find interesting: -
a.nationalauditprojects.org.uk/NAP4_home
b.das.uk.com/content/video/…
c.vortexapproach.org
If you have any others of interest, tweet them to us for inclusion next time!
#JanuAirway 8/16
a.nationalauditprojects.org.uk/NAP4_home
b.das.uk.com/content/video/…
c.vortexapproach.org
If you have any others of interest, tweet them to us for inclusion next time!
#JanuAirway 8/16
#JanuAIRWAY - Airway Pharmacology
Knowledge of what drugs we can use and how we use them in airway management is indispensable – especially where planning is concerned. Here’s a #OnePager that covers the essentials 9/16
Knowledge of what drugs we can use and how we use them in airway management is indispensable – especially where planning is concerned. Here’s a #OnePager that covers the essentials 9/16
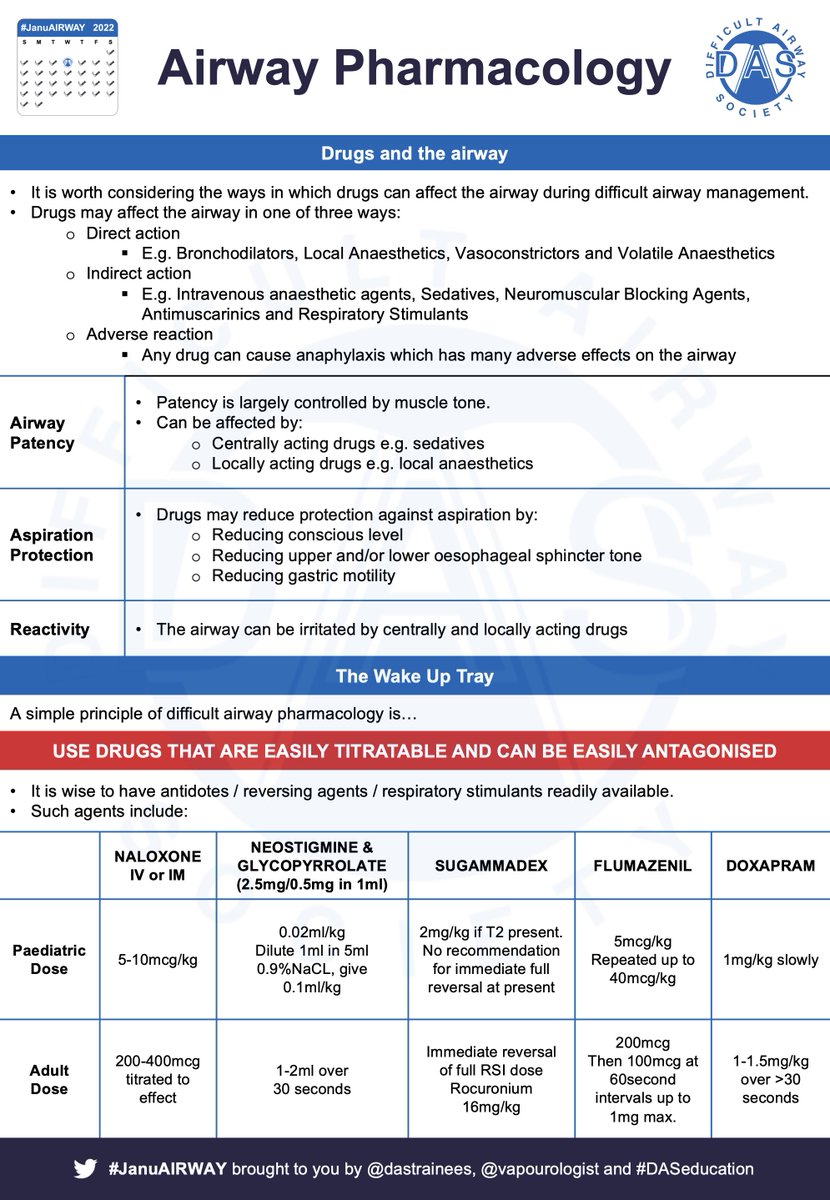
#JanuAirway Drugs affect the airway in one of three ways: -
1) Direct action e.g. local anaesthetics or bronchodilators
2) Indirect action e.g. volatile anaesthetics or respiratory stimulants
3) Adverse reaction e.g. as a result of anaphylaxis
10/16
1) Direct action e.g. local anaesthetics or bronchodilators
2) Indirect action e.g. volatile anaesthetics or respiratory stimulants
3) Adverse reaction e.g. as a result of anaphylaxis
10/16
#JanuAirway 3 main effects drugs have on the airway are be changing: -
Airway patency – usually by reducing muscle tone
Airway reactivity – irritation by central or local effects
Aspiration protection – reduced (e.g. drugs reducing conscious level) or improved (e.g. PPI)
11/16
Airway patency – usually by reducing muscle tone
Airway reactivity – irritation by central or local effects
Aspiration protection – reduced (e.g. drugs reducing conscious level) or improved (e.g. PPI)
11/16
#JanuAirway Drug controversies in difficult airways: -
•To paralyse or not
•Spont Vent or IPPV during induction of anaesthesia
Here’s a #OnePager
Key points: -
•Paralysis is not irreversible – have a plan
•Maintaining spontaneous ventilation can be inconsistent
12/16
•To paralyse or not
•Spont Vent or IPPV during induction of anaesthesia
Here’s a #OnePager
Key points: -
•Paralysis is not irreversible – have a plan
•Maintaining spontaneous ventilation can be inconsistent
12/16

#JanuAirway 2 simple rules for drugs: -
1) Use drugs that are easily titratable & reversible
2) Plan for failure
@vapourologist uses a ‘wake up tray’ with NRDS drugs drawn up/ready to go
N – Naloxone
R – Reversal (Glyc/Neostig)
D – Doxapram
S – Sugammadex (if applicable)
13/16
1) Use drugs that are easily titratable & reversible
2) Plan for failure
@vapourologist uses a ‘wake up tray’ with NRDS drugs drawn up/ready to go
N – Naloxone
R – Reversal (Glyc/Neostig)
D – Doxapram
S – Sugammadex (if applicable)
13/16
#JanuAirway 2 main drugs: - 1) sedatives & 2) local anaesthetics – Key is that local needs to be in the right place, but you don’t need much. This is @vapourologist after gargling 10ml instilagel with 10ml water for 2 mins. More about this on the ATI day! 14/16
Here are some papers / links that you might find interesting: -
a.pubmed.ncbi.nlm.nih.gov/21436166/
b.
c.pubmed.ncbi.nlm.nih.gov/23512191/
If you have any others of interest, tweet them to us for inclusion next time!
#JanuAirway 15/16
a.pubmed.ncbi.nlm.nih.gov/21436166/
b.
c.pubmed.ncbi.nlm.nih.gov/23512191/
If you have any others of interest, tweet them to us for inclusion next time!
#JanuAirway 15/16
Hope that helps. Tomorrow we'll look at Basic Airway Equipment. See you then! #JanuAirway 16/16
*Disclaimer: Inclusion of content (equipment, techniques and scoring systems etc.) in #JanuAIRWAY does not constitute DAS endorsement
*Disclaimer: Inclusion of content (equipment, techniques and scoring systems etc.) in #JanuAIRWAY does not constitute DAS endorsement
• • •
Missing some Tweet in this thread? You can try to
force a refresh