Thanks to the 1000's of people who have powered our 3rd dose effort. We've made amazing progress in a short time—and still have further to go.
A thread on why 3+ doses continues to be important and where we need to focus 🧵
A thread on why 3+ doses continues to be important and where we need to focus 🧵

We now have more real world data showing that 3 doses is better than 2 at preventing infection and serious illness with Omicron
These two slides were shared by Dr. Allison McGeer and summarize data on infection and hospitalization with 3 v 2 doses in the UK
These two slides were shared by Dr. Allison McGeer and summarize data on infection and hospitalization with 3 v 2 doses in the UK


Older adults are most at risk of COVID complications and thankfully we've done a pretty good job at getting vaccines to those 70+
But some regions are lagging behind. What can we learn from regions where vaccination rates are higher?
But some regions are lagging behind. What can we learn from regions where vaccination rates are higher?

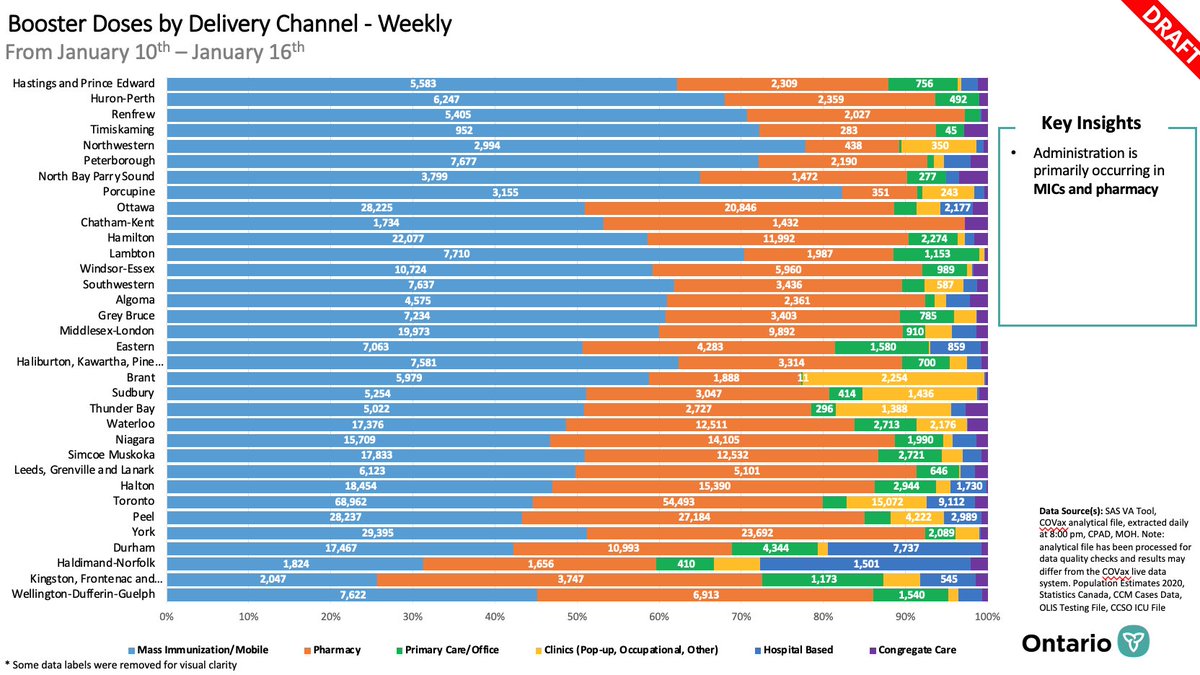
This slide illustrates that the variation in 3rd dose vaccination rates by public health unit is not about which delivery channels are used—the factors are likely more complex and worth unpacking
We need to increase uptake now for those <70
And in particular we need to focus on priority populations
Pregnant people are at high risk of complications if they get COVID, yet only 17% have received a 3rd dose
People who are immunocompromised need 3rd AND 4th doses
And in particular we need to focus on priority populations
Pregnant people are at high risk of complications if they get COVID, yet only 17% have received a 3rd dose
People who are immunocompromised need 3rd AND 4th doses

Who is eligible for a 4th dose?
4th doses can be given 3 months after a 3rd dose for people with very weak immune systems, for example, b/c of dialysis, cancer treatment, or meds that weaken the immune system including high-dose steroids 👇🏽
dfcm.utoronto.ca/sites/default/…
4th doses can be given 3 months after a 3rd dose for people with very weak immune systems, for example, b/c of dialysis, cancer treatment, or meds that weaken the immune system including high-dose steroids 👇🏽
dfcm.utoronto.ca/sites/default/…

3 doses is still important even if you had COVID
Our experience with previous variants tell us that even after infection with COVID, vaccines add stronger and longer lasting protection. This means less chance of re-infection or transmission to others
Our experience with previous variants tell us that even after infection with COVID, vaccines add stronger and longer lasting protection. This means less chance of re-infection or transmission to others
If you got COVID, when should you get your 3rd dose?
You can receive it as soon as your symptoms are gone but most infectious disease experts recommend waiting 4-8 weeks to get stronger longer-lasting immunity
You can receive it as soon as your symptoms are gone but most infectious disease experts recommend waiting 4-8 weeks to get stronger longer-lasting immunity
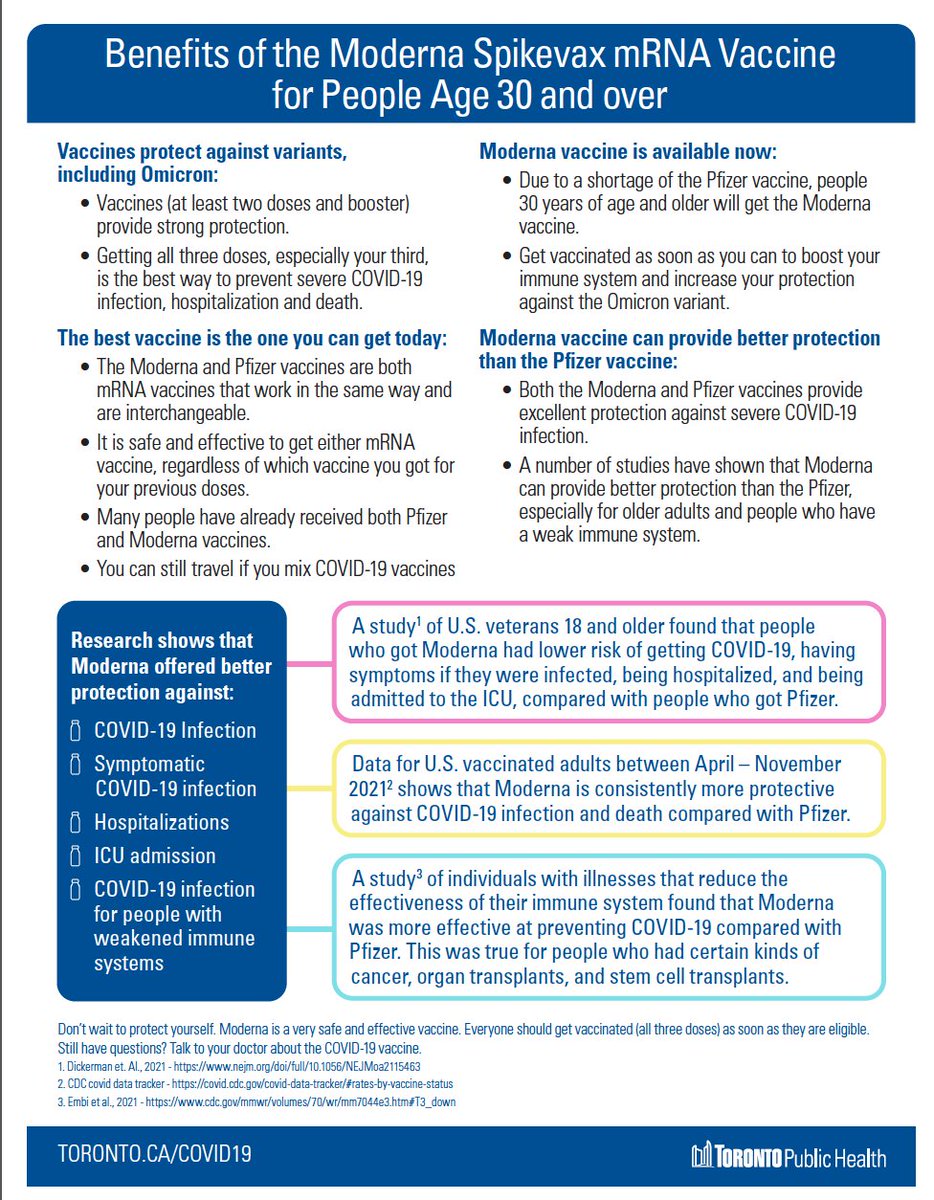
Finally, either Moderna or Pfizer are good choices for your 3rd dose if you are age 30+. Both are mRNA vaccines and have pretty much the same ingredients. Mixing and matching is just fine.
This is 1-pager from @TOPublicHealth provides more detail
track.upaknee.com/c/443/06c5e9b8…
This is 1-pager from @TOPublicHealth provides more detail
track.upaknee.com/c/443/06c5e9b8…
We need continue to use many layers of protection to keep ourselves and more vulnerable people in the community safe and reduce our risk of serious outcomes from COVID-19.
Vaccination with a 1st/2nd/3rd/4th dose is one of the most important layers of protection we have
Vaccination with a 1st/2nd/3rd/4th dose is one of the most important layers of protection we have
• • •
Missing some Tweet in this thread? You can try to
force a refresh