/1 Hi Lucy and your colleagues.
Your advocacy toolkit contains poorly sourced, contexted, and biased information on mental health during the pandemic/schooling.
And I have receipts too!
(thread)
#urgencyofnormal
Your advocacy toolkit contains poorly sourced, contexted, and biased information on mental health during the pandemic/schooling.
And I have receipts too!
(thread)
#urgencyofnormal
https://twitter.com/drlucymcbride/status/1485810134689460229
/2 I'm skipping the first line (for now), but the second part, about "deaths from child suicide vastly outnumbering deaths from COVID and are increasing" is about as awful as it gets. I consider it ghoulish to wield child suicide statistics inaccurately to make advocacy points. 

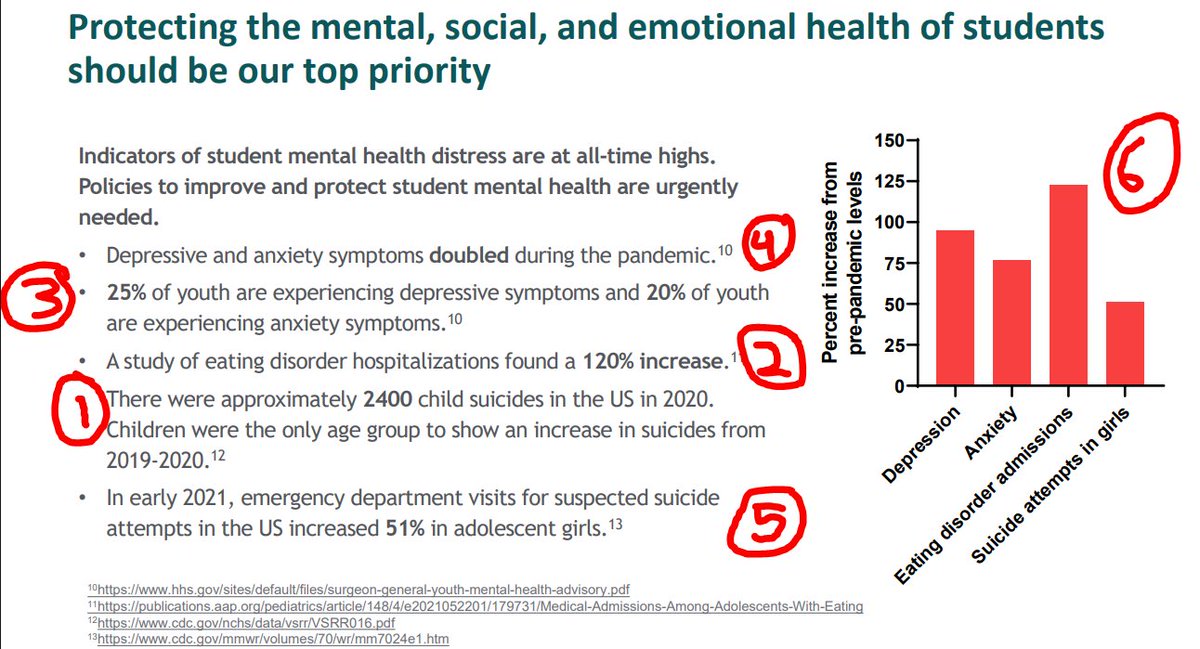
/3 In order, I'm going to go through your awful slide on mental health as you selectively cited "scary findings." Of course, as the suicidologist, I'm going to start with your clearly expert-free statement on child suicides in the US, as this is my expertise.

/4 You cite 2400 child suicides in the US for 2020, which is an overestimate by 10.2%. We have CDC wonder and can clearly see that there were 2,177 suicides in the "under 18" group, and 1,679 in the "under 17 group."


/5 Was it an increase from 2020? It would not be accurate to describe it this way.
Ive done things that are important in comparing yearly suicides:
* convert to rate per 100,000
* show error bars to demonstrate signiificant change
* use data honestly with context
Ive done things that are important in comparing yearly suicides:
* convert to rate per 100,000
* show error bars to demonstrate signiificant change
* use data honestly with context
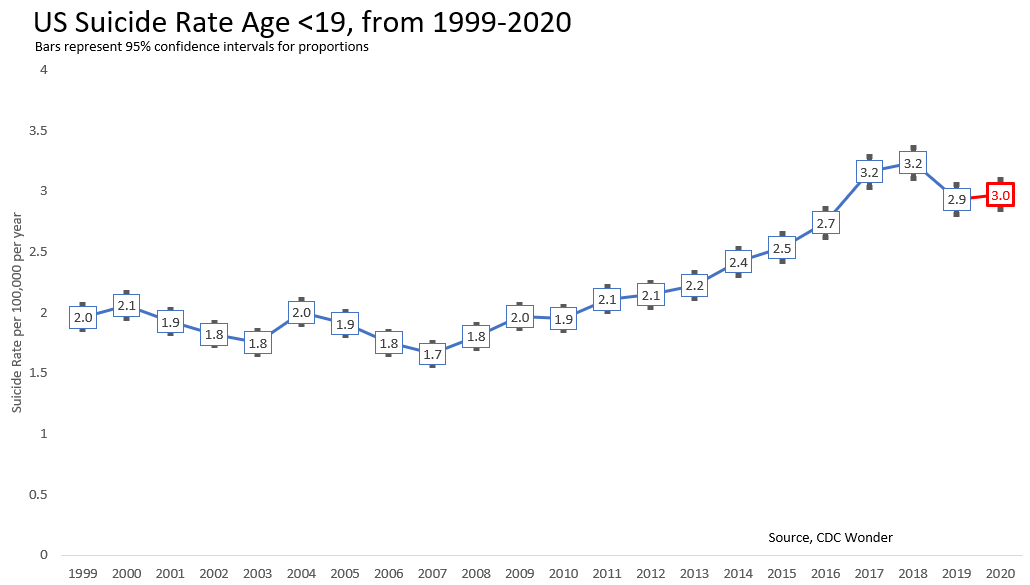
/6 You & your colleagues missed something very important in your inaccurate and sensationalistic reporting.
Both 2019 & 2020 are SIGNIFICANTLY lower than 2018.
Sometimes though, we cite things and the citation source made a mistake.
Both 2019 & 2020 are SIGNIFICANTLY lower than 2018.
Sometimes though, we cite things and the citation source made a mistake.
/7 But this is academic misconduct. You have mis-cited the CDC report. I don't care if its an oversight, it's unacceptable.
Not only were children NOT the only age to show increase (25-34 did as well in males), NO CHILD GROUP SHOWED A SIGNIFICANT INCREASE. The citation says so.
Not only were children NOT the only age to show increase (25-34 did as well in males), NO CHILD GROUP SHOWED A SIGNIFICANT INCREASE. The citation says so.


/8 But, lets follow the logic of your summary slide. In 2019 there were 2,156 suicides 0-18 years. And 2020 there were 2,177. That's 19 extra suicides. So 19 extra suicides vs 179 covid deaths in 2019 (Source: AAP).
/9 But I hope for the sake of the kids you all see as pediatricians (and one child psychiatrist who either did not know how to interpret the evidence or wasn't listened to) you don't do this "fewer kids died of X vs Y so X isn't really a concern" thing. That's pretty ghoulish.
/10 For thoroughness:
* ages <15 (2019 is the non-significant outlier not 2020)
* ages 15-18 (34 fewer suicides! so by your logic... schools out?)
* girls
* non-white - most signal but still not statistically different and it looks more like 2019 the outlier year.
* ages <15 (2019 is the non-significant outlier not 2020)
* ages 15-18 (34 fewer suicides! so by your logic... schools out?)
* girls
* non-white - most signal but still not statistically different and it looks more like 2019 the outlier year.




/11 And as I've demonstrated before, when ALL KIDS EXPERIENCED SCHOOL CLOSURES in the US, there was, for the first time in history, a flattening of suicide risk during school months.
https://twitter.com/tylerblack32/status/1470785708394754052
/12 So now that I've debunked your claim about suicides increasing, shown that you improperly cited your narrative-selected citation, and demonstrated that school closures were associated with less risk, you'll update your advocacy, right?
Because this is about evidence, right?
Because this is about evidence, right?
/13 OK Let's move to #2.
Undoubtedly, I feel that the impact of the pandemic on eating disorders (ED) is the area with strongest evidence. Of course, you neglected to show that increases ED admissions didn't slow when schools opened. MI hybridized Sept 2020 and opened Dec 21.
Undoubtedly, I feel that the impact of the pandemic on eating disorders (ED) is the area with strongest evidence. Of course, you neglected to show that increases ED admissions didn't slow when schools opened. MI hybridized Sept 2020 and opened Dec 21.

/14 Eating disorder side-note: I'm not an ED specialist, but I believe the pandemic has hurt ED kids, due to lack of "healthy ways to mask an ED" (gyms, sports), lead-time bias (more time to display disordered eating and be detected), & global (not just school) lifestyle changes)
/15 A large collaborative multi-national study has found variable effects of lockdown on eating disorders, and I do not believe that after all the data has been completed, it will be simply summed "lockdown made eating disorders worse."
mdpi.com/2072-6643/14/1…
mdpi.com/2072-6643/14/1…

/16 OK so in Number 3, you cite the HHS report that plainly states your point.
However, you (And the HHS) neglected to accurately describe Racine et al, which is the source of this figure..
However, you (And the HHS) neglected to accurately describe Racine et al, which is the source of this figure..

/17 Racine et al found the 25% depressive / 20% figure, however when they removed low-quality studies (21 of 26!), they arrived at much lower figures for depression, (18%, 11% to 26%) and anxiety (12%, 7% to 20%)


/18 As well, they commented on the severe heterogeneity (the studies were wildly different suggesting poor quality and severe confounding). Their final estimate for depressive symptoms (21% to 30%) was incompatible INCLUDING CONFIDENCE INTERVAL with 18 of 26 included studies.

/19 So like my criticism for the @HHSGov , you don't escape it either. If you're going to cite an article, read it and critically report what it's saying. (@vivek_murthy I really respect you, but you might really benefit from reading this thread and comparing it to your report)
/20 Well i guess that tackles #4 as well, doesn't it? It's the same citation.
The "doubling" is more accurately "by selecting high quality studies, there may have been an increase in anxiety and depression prevalence but it was not outside of previous confidence intervals."
The "doubling" is more accurately "by selecting high quality studies, there may have been an increase in anxiety and depression prevalence but it was not outside of previous confidence intervals."

/21 #5... Oh, my favourite MMWR, where the authors confused "suspected severe attempt" from NSSI, and did so on the basis of a paper on older adults showing that NSSI is a small proportion of ED self-harm presentations (please, @CDCgov, use child & youth mental health experts).

/22 I don't need to do a tweet thread criticizing this, because I ALREADY DID IT MONTHS AGO.
Here:
and here:
Here:
https://twitter.com/tylerblack32/status/1403418823751962630
and here:
https://twitter.com/tylerblack32/status/1471525557611474947
/23 Finally, you did this awful thing at 6, YOU CANT DO THAT. A horrid graph and you should be embarrassed to have produced it
There are no error bars. These are not nationally representative samples (except for suicide attempts). Pre-pandemic levels have error bars too.
There are no error bars. These are not nationally representative samples (except for suicide attempts). Pre-pandemic levels have error bars too.
/24 As well, Racine et al were looking at *symptoms of anxiety* and your "pre-pandemic" figures come from epidemiological studies of DISORDER rates.
Again, I'm going to attribute this to incompetence/biased thinking but it borders on academic and scientific malpractice.
Again, I'm going to attribute this to incompetence/biased thinking but it borders on academic and scientific malpractice.
/25 I've made your graph better and more accurate, because what we all care about most is not your advocacy point and prior beliefs, but using evidence to inform advocacy and decision-making.

/26 Besides, if I was arguing about returning to schools, personally, I wouldn't be citing evidence that talks about "the pandemic" and doesn't actually disambiguate pandemic distress from school distress.
This bait-and-switch all too common amongst unscientific ideologues.
This bait-and-switch all too common amongst unscientific ideologues.
/27 So, in total, your slides on mental health are beyond bad. By being unscientific and biased in your selection and presentation of data, you are part of the misinformation crisis of this pandemic.
/28 Oh, and shout out to @vivek_murthy @CDCgov @HHSGov I am available to consult on topics of child and youth mental health. I care the most about good science and science communication, and removing moral panic/poor science from policy discussion.
/29 This is the new me - less snark, more pointed, data driven. I hope threads like this go as viral as my snarky one, because I want to be less snarky.
2020. whenever :P time is a circle
• • •
Missing some Tweet in this thread? You can try to
force a refresh