***********
Canadian Suicidology Update
***********
We have official @StatCan_eng suicide data for 2020, ready to analyse by year. This lets us look at the trends and to see whether or not the "pandemic year" was associated with any significant changes, by gender and age.
/1
Canadian Suicidology Update
***********
We have official @StatCan_eng suicide data for 2020, ready to analyse by year. This lets us look at the trends and to see whether or not the "pandemic year" was associated with any significant changes, by gender and age.
/1

The headline is the MASSIVE drop in suicide rates during the first year of the pandemic. While not as massive as suggested in McIntyre et al*, it's still huge and significant:
DOWN 17.6% in males and 12.5% in females. 16.4% overall.
/2
DOWN 17.6% in males and 12.5% in females. 16.4% overall.
/2

I can break down our age groups as well, to look at specific groupings.
CANADIANS 65+
For older Canadians, both decreases (men down 14%, women down 6%) are no longer statistically significant (super close for the 65+ men).
/3
CANADIANS 65+
For older Canadians, both decreases (men down 14%, women down 6%) are no longer statistically significant (super close for the 65+ men).
/3

CANADIANS 40-64:
Both Canadian men and women 40-64 had massive decrease in suicide rates, drops not seen in the past 2 decades. a whopping 20% decrease in both groups, and the lowest rate of suicide recorded in the past 21 years.
/4
Both Canadian men and women 40-64 had massive decrease in suicide rates, drops not seen in the past 2 decades. a whopping 20% decrease in both groups, and the lowest rate of suicide recorded in the past 21 years.
/4

CANADIAN THIRTYSOMETHINGS:
Neither significant, but there was a split in which men suicide rates decreased & women increased. However, both rates are entirely consistent with overall trends, so before you get all "i wonder if it's because..." it's stats... they do this.
/5
Neither significant, but there was a split in which men suicide rates decreased & women increased. However, both rates are entirely consistent with overall trends, so before you get all "i wonder if it's because..." it's stats... they do this.
/5

CANADIANS IN THEIR 20'S:
At the 20-29 group, decreases seen once more, statistically significant for Canadian men (largest drop on record @ 17% lower), and a 6-year-low for women at 6.8 per 100,000.
/6
At the 20-29 group, decreases seen once more, statistically significant for Canadian men (largest drop on record @ 17% lower), and a 6-year-low for women at 6.8 per 100,000.
/6

CANADIAN KIDS OVERALL:
Under 20, because thankfully suicides much rarer in kids, the data is a bit noisier. None of the changes are significant in 2020 compared to 2019, but it is important to note that for Canadian boys, the rate is WAY lower than 2018's rate.
/7
Under 20, because thankfully suicides much rarer in kids, the data is a bit noisier. None of the changes are significant in 2020 compared to 2019, but it is important to note that for Canadian boys, the rate is WAY lower than 2018's rate.
/7

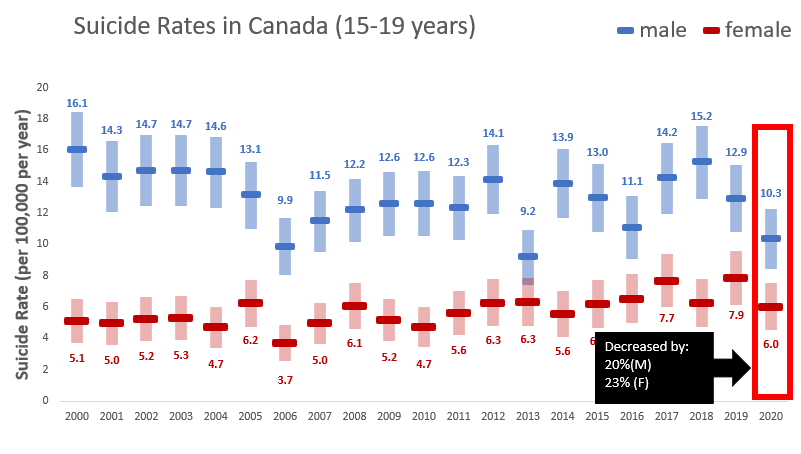
CANADIAN KIDS 15-19:
Again huge drops by %, though neither statistically significant compared to 2019. Both boys and girls 15-19 years of age had a suicide rate decrease of more than 20%
Again huge drops by %, though neither statistically significant compared to 2019. Both boys and girls 15-19 years of age had a suicide rate decrease of more than 20%
CANADIAN KIDS <15 YEARS:
For young Canadian kids, there was no meaningful change of what is already best described as very noisy data.
For young Canadian kids, there was no meaningful change of what is already best described as very noisy data.

(For people interested in such things, every jurisdiction in Canada had some form of school lockdown at some point for a significant chunk of 2020)
Overall, this is conclusive evidence that in Canada, suicide rates did not increase in the first year of the pandemic. There was no significant increase in any group broken down by age bands or sex.
Many age+sex groups set 6,10, or sometimes 21 year lows.
Many age+sex groups set 6,10, or sometimes 21 year lows.
Statistics Canada does NOT report race-based mortality data, so we would need the @StatCan_eng crew to delve into their data to determine if there were differences within minority populations (PLEASE DO!!)
Please feel free to use this thread if you are talking about Canadian suicide information in the pandemic. Media, I'm available for contact at dr.tylerblack at gmail dot com.
* McIntyre reported -32%, and there is no way this number is correct. I'm pretty sure I know the table he relied on now (13-10-0810-01 @statcan_eng) and that's disappointing.
Suicide data has up to a years lag in Canada and a cursory glance at the table when it was cited in Feb 2021 would have clearly shown that. I've contacted the editor @EditorJRSM @KamranAbbasi by email.
Whenever I've been interviewed about it, I would say something like "the number is so remarkably low it makes me worried that they used data that is lagged" and ... well... they did. Paper needs major revision. Rate severely underreported (7.3 vs 10.1 actual, 10.6 age standard)
• • •
Missing some Tweet in this thread? You can try to
force a refresh