
🧵 Long COVID Part 1: This problematic paper
This paper by Borch et al is getting a lot of attention and is being cited as evidence that LongCOVID in kids is rare and of short duration. I don't think that's what it shows.
(1/23)
link.springer.com/article/10.100…
This paper by Borch et al is getting a lot of attention and is being cited as evidence that LongCOVID in kids is rare and of short duration. I don't think that's what it shows.
(1/23)
link.springer.com/article/10.100…
The part 2 🧵 will discuss a major conceptual flaw of such enquiries but first let's deal with this paper.
I'd normally deal with the methodological issues first and then matters of presentation of the results and conclusions but there are some egregious issues here.
(2/23)
I'd normally deal with the methodological issues first and then matters of presentation of the results and conclusions but there are some egregious issues here.
(2/23)
In the abstract the authors say
'A nationwide cohort study of 37,522 children aged 0–17 years with RT-PCR verified SARS-CoV-2 infection (response rate 44.9%) and a control group of 78,037 children (response rate 21.3%).' (directly copied)
But this is very misleading.
(3/23)
'A nationwide cohort study of 37,522 children aged 0–17 years with RT-PCR verified SARS-CoV-2 infection (response rate 44.9%) and a control group of 78,037 children (response rate 21.3%).' (directly copied)
But this is very misleading.
(3/23)
This is a case control study that identified two groups of children and sent a questionnaire to them and/or their parents. There is no study cohort here.
The numbers cited here are those of the questionnaires sent out, not the questionnaires received or included.
(4/23)
The numbers cited here are those of the questionnaires sent out, not the questionnaires received or included.
(4/23)
So this looks like a study of >100,000 kids as some have noted but actually 16836 questionnaires were received in the COVID group and 16642 in the control group, final numbers being 15041 and 15080. Still substantial but not >100,000.
(5/23)
(5/23)
https://twitter.com/BallouxFrancois/status/1487139909349654528?s=20&t=F4VMG-iCJZ4Tu2S9Yk8TFQ
Key result in the abstract:
'Symptoms lasting > 4 weeks were common among both SARS-CoV-2 children and controls. However, SARS-CoV-2 children aged 6–17 years reported symptoms more frequently than the control group (percent difference 0.8%).'
More on this later.
(6/23)
'Symptoms lasting > 4 weeks were common among both SARS-CoV-2 children and controls. However, SARS-CoV-2 children aged 6–17 years reported symptoms more frequently than the control group (percent difference 0.8%).'
(6/23)
The authors designed a questionnaire for each group & the questionnaires are very similar in that they ask about the experience and duration of a set of symptoms in both groups.
(For the questionnaires & the data I have used below, please see the supplementary materials)
(7/23)
(For the questionnaires & the data I have used below, please see the supplementary materials)
(7/23)
The key difference is that the COVID group questionnaire asks about a set of symptoms following PCR-confirmed COVID, whereas the control questionnaire asks for the same symptoms at any point in the *last year*.
(8/23)
(8/23)
Crucially it does not ask if the symptoms occurred during a period of acute illness or in relation to chronic illnesses that the child has (5% in both groups endorsed a chronic illness). If the symptoms occurred during an acute illness they should be excluded.
(9/23)
(9/23)
So what we have is a comparison of symptoms between children who had COVID and have had symptoms since the infection, and kids who did not have COVID but may have had other illnesses in the last year, namely the period of enquiry.
(10/23)
(10/23)
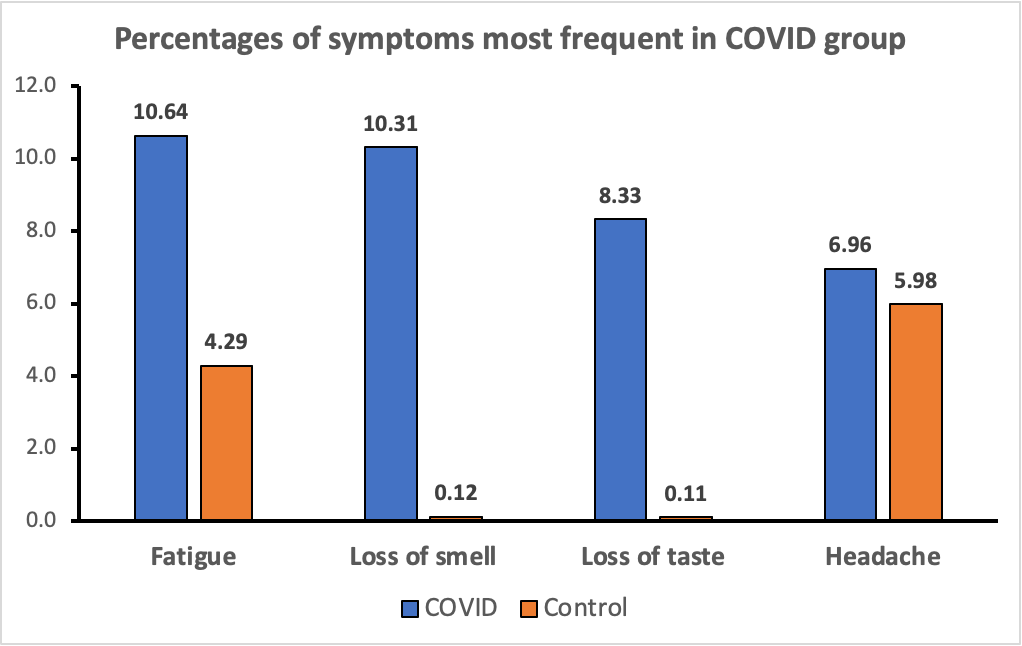
The analysis is mainly in terms of individual symptoms (more on this in Part 2) i.e. comparing the prevalence of each symptom between the two groups. Here is the key figure from the paper showing the risk difference (a measure of the difference in proportions b/w groups)
(11/23)
(11/23)

You can see that some key symptoms such as loss of taste and loss of smell are more common in the COVID group. I've plotted the data here (0-17 yrs) in terms of the percentages to give a clear sense of this, first in terms of the symptoms most common in the COVID group.
(12/23)
(12/23)
Here's the same plot for the symptoms most common in the control group, the scales on both graphs are the same and fatigue features here as well.. Important to remember that in the control group these are symptoms experienced at any point in the last year.
(13/23)
(13/23)

I forgot to include muscle weakness (2.51% in COVID group, 0.71 in controls) and dizziness (3.41 vs 1.23).
Finally here are the percentages in terms of number of symptoms, again 0-17 years.
You'll see here that the difference between the two groups is 3.09%.
(14/23)
Finally here are the percentages in terms of number of symptoms, again 0-17 years.
You'll see here that the difference between the two groups is 3.09%.
(14/23)

So where does the 0.8% come from? I don't have the raw data to calculate this but according to what the authors state is that this is the difference between 'any symptoms' in the 6-17 group, that in the 0-5 groups actually being 2.8% higher in the controls.
(15/23)
(15/23)
Ok, that's the data, please feel free to check my graphs, I've included the data labels for exactly that purpose.
So what does this study tell us?
(16/23)
So what does this study tell us?
(16/23)
What we have here is a comparison of the prevalence of individual symptoms in children who have had COVID to the prevalence of those symptoms over the last year in children who have not had COVID but may or may not have had other illnesses during that period.
(17/n)
(17/n)
I hope it is clear why this is a flawed comparison just based on this major limitation of symptom ascertainment in the control group.
However, even accounting for this, the data on the more specific symptoms like loss of taste and loss of smell is striking.
(18/23)
However, even accounting for this, the data on the more specific symptoms like loss of taste and loss of smell is striking.
(18/23)
Remember this is all about symptoms persisting for more than 4 weeks. Further, when you look at kids experiencing 2 or more symptoms, the percentages are higher in the COVID group. I haven't run any stats on these as I don't have the raw data for the appropriate analysis.
(19/23)
(19/23)
And the appropriate analysis would be to look at clusters of co-occurring symptoms, not the prevalence of individual symptoms.
I do think this is a problematic paper and even accounting for these problems, the findings are not really reassuring.
(20/23)
I do think this is a problematic paper and even accounting for these problems, the findings are not really reassuring.
(20/23)
Final point and this is a key one. This paper is not about LongCOVID, it is about the comparative prevalence of individual symptoms that have been noted to be persistent after COVID infection. There is no definition of LongCOVID used or operationalised in the study.
(21/23)
(21/23)
So what it tells us about LongCOVID is limited.
However the paper does make strong claims about Long COVID and very troublingly, repeatedly refers to 'long COVID' (i.e. in quotes).
In the next thread I'm going to elaborate on the key conceptual problem.
(22/23)
However the paper does make strong claims about Long COVID and very troublingly, repeatedly refers to 'long COVID' (i.e. in quotes).
In the next thread I'm going to elaborate on the key conceptual problem.
(22/23)
And if you feel you have not suffered enough, here is the link to the next part.
https://twitter.com/HZiauddeen/status/1487247912719597569?s=20&t=F4VMG-iCJZ4Tu2S9Yk8TFQ
• • •
Missing some Tweet in this thread? You can try to
force a refresh


