Someone sent this to me earnestly, but, honestly, if it weren't convincing parents to not vaccinate their kids :(
To someone with a medical background and actually...you know... Relevant statistical and educational experience... All of these comments laughable.
Sigh.
To someone with a medical background and actually...you know... Relevant statistical and educational experience... All of these comments laughable.
Sigh.




My spit take moment

Vaccinating children who got control (100% of enrolled parents wanted their children to get vaccinated! It was a voluntary study!) is supremely ethical. Vaccines save lives even covid vaccines and youngest lives. This awful beast turns the **best decision of the RCT** into evil.

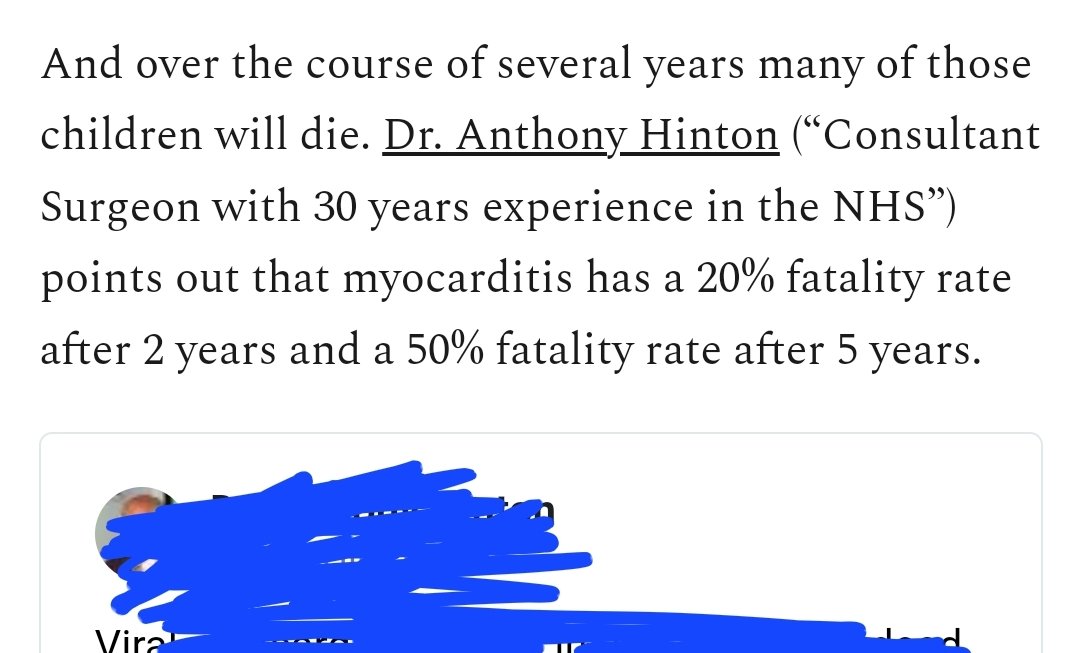
Dr. Anthony Hinton, consultant surgeon with 30 years of experience in the NHS is obviously extremely unaware of pediatric statistics of myocarditis blood work detections in pediatrics, including after athletic events.
You can literally say all of the same things by saying "I graduated with an arts degree and did a PhD in political economy".
It's well understood that millions of undergrads/grads are FORCED to take statistics courses for their degrees. None are experts in statistics.
It's well understood that millions of undergrads/grads are FORCED to take statistics courses for their degrees. None are experts in statistics.

• • •
Missing some Tweet in this thread? You can try to
force a refresh