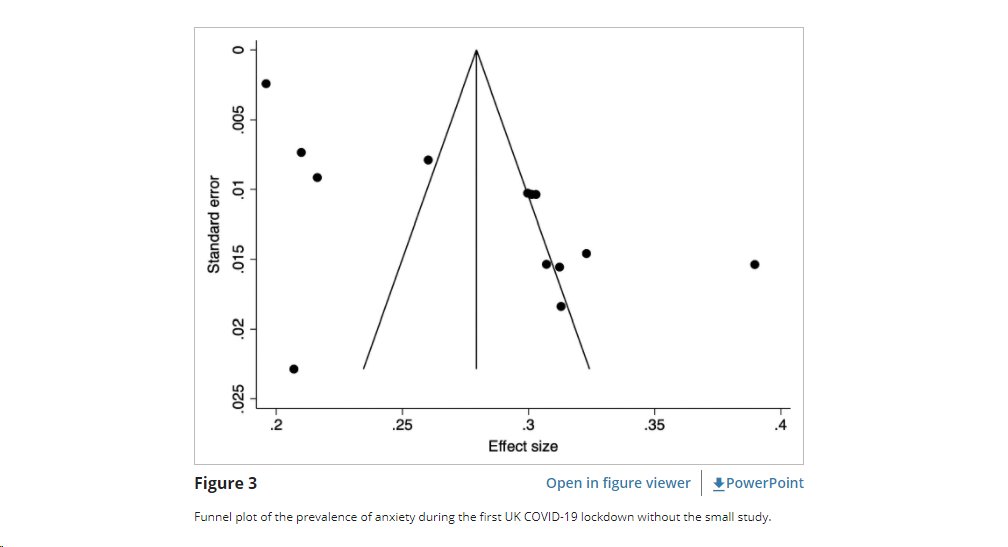
Reviewing a PUBLISHED PEER REVIEWED paper about anxiety prevalence during the pandemic in the UK, and the authors commented that because this funnel plot is symmetrical, publication bias is unlikely.
NONE OF THE STUDIES ARE IN THE FUNNEL!!!!!
NONE OF THE STUDIES ARE IN THE FUNNEL!!!!!

Funnel plots are supposed to give you confidence that the estimate is not biased. Usually, it's to "show you if there is a bias around the mean."
In this case, the funnel plot serves to tell us to simply throw out the effect size.
In this case, the funnel plot serves to tell us to simply throw out the effect size.
As the error gets smaller, the certainty range is supposed to get smaller, that's the entire point of the funnel plot.
This is simply a metaanalysis of randomness.
This is simply a metaanalysis of randomness.
i can't even :( ...
so few of the CONFIDENCE INTERVALS for any of the studies even overlap, let alone agree with the estimate.
this one is for "depression"
so few of the CONFIDENCE INTERVALS for any of the studies even overlap, let alone agree with the estimate.
this one is for "depression"

but don't worry, "Due to the high heterogeneity, random-effects models were used in the analysis of the findings."
sigh.
Are we ever going to have sound epidemiological publications in pandemic mental health research?
sigh.
Are we ever going to have sound epidemiological publications in pandemic mental health research?
this is totally normal (they removed the "small outlier study" to make the above plot, despite it being a survey of 600, even though there are other surveys they didn't remove with 315 participants)

well at least its "symmetrical" - no publication bias!!!!!!!
how on earth does this stuff get published
how on earth does this stuff get published

for reference, this is what funnel plots are SUPPOSED to look like (both showing bias and not)

• • •
Missing some Tweet in this thread? You can try to
force a refresh