USA Suicidology Update, 2020-2021
********
I can now create a 2021 provisional estimate, with error, for the suicide rates for 2021. My method will be described at the end of the thread.
Contrary to the #moralpanic 2020-2021 suicide rates did NOT increase.
/1
********
I can now create a 2021 provisional estimate, with error, for the suicide rates for 2021. My method will be described at the end of the thread.
Contrary to the #moralpanic 2020-2021 suicide rates did NOT increase.
/1

The rate for both males and females in the United States will likely be within the expected fluctuation of the previous years, and still less than the "peak" of 2018 pre-pandemic.
/2
/2
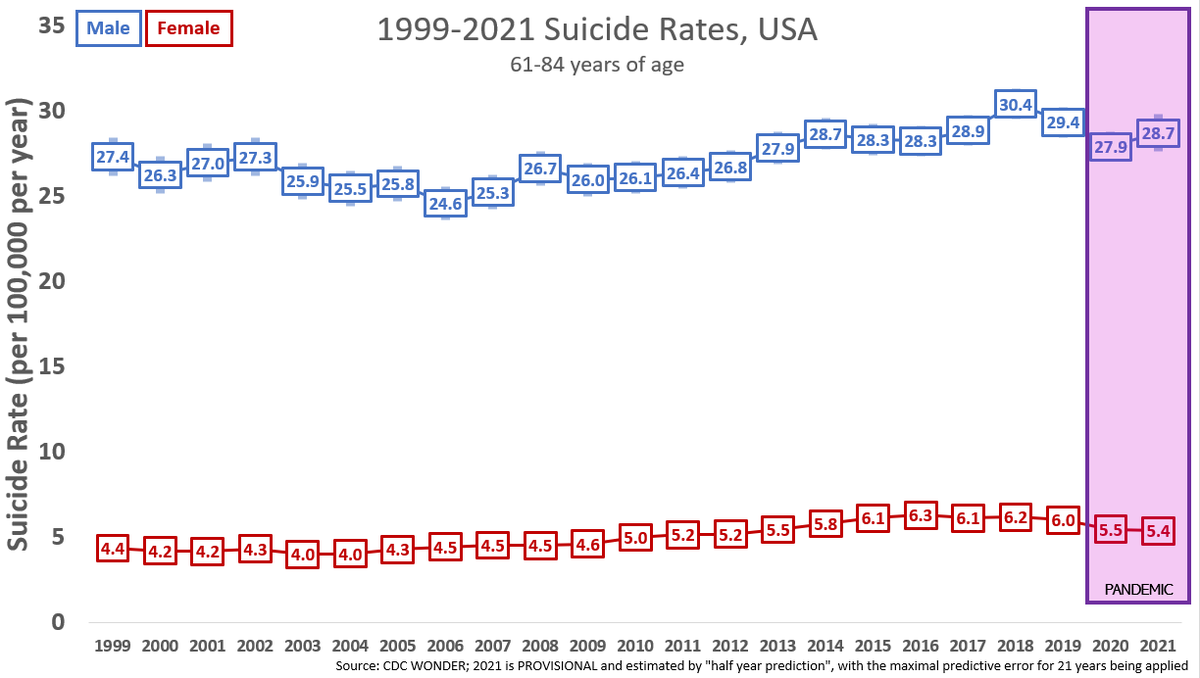
For Adults 61-84, likely a slight uptick for men but within 2019 levels, and for women no overall change.
/3
/3
For adults 41-60, the significant drop seen in 2020 will likely continue for both men and women.
/4
/4

For adults 25-40, no changes are significant but there seems to be a continuing and increase of about 2.5% per year in the male rate since 2009.
/5
/5

For YOUNG ADULTS (18-24), **please note that neither change is outside of the error prediction so this is best described as** no significant differences. If the point estimates hold, they will both be highs. However, neither increase unprecedented or "A TSUNAMI" if they hold.
/6
/6

For PEDIATRIC POPULATION (0-17), **please note that neither change is outside of the error prediction so this is best described as** no significant differences. Even if the point estimates hold, none of these increases unprecedented or "A TSUNAMI".
/7
/7

All-in-all, its looking like 2021 will be a mundane year for final suicide numbers. In the coming days I will do my best to take a peek at the racial divides.
/8
/8
"2021 ERROR SIZE"
I ran a model in which all the previous "Jan thru June" rates were compared to that year's final rate, to get the most conservative (largest) error in this prediction.
For the second year in a row, the "TSUNAMI OF SUICIDE" moral panic will not test true.
/9
I ran a model in which all the previous "Jan thru June" rates were compared to that year's final rate, to get the most conservative (largest) error in this prediction.
For the second year in a row, the "TSUNAMI OF SUICIDE" moral panic will not test true.
/9
"2021 Provisional Rate"
The 2021 rate is then displayed as the Jan-June rate (adjusted to to increase by 2.6% when provisional to final, based off of previous CDC Wonder updates), with the error bars above.
/10
The 2021 rate is then displayed as the Jan-June rate (adjusted to to increase by 2.6% when provisional to final, based off of previous CDC Wonder updates), with the error bars above.
/10
• • •
Missing some Tweet in this thread? You can try to
force a refresh