30 bad COVID arguments debunked: thelogicofscience.com/2022/01/19/deb…
These are so frequent & so soundly rebuffed, I'm putting them all on here because you can't be trusted to click on link. Skip the next 30 if you're so over this right now.
A thread.
These are so frequent & so soundly rebuffed, I'm putting them all on here because you can't be trusted to click on link. Skip the next 30 if you're so over this right now.
A thread.


This one really annoys me because somehow it's 'ok' for people with co-morbidities to die. It also assumes co-morbidities are somehow constantly threatening your life instead of being an intermittent inconvenience. You have asthma? You're co-morbid. Migraines? Co-morbid. 
That is the whole point of a vaccine. To stay healthy. This is why every modern society recommends vaccinating children. We even vaccinate our bloody dogs to stop them dying and my Labrador eats rotten eggs out of the neighbour's compost.
Your immune system doesn't trust you; that's why it wants you to be vaccinated.




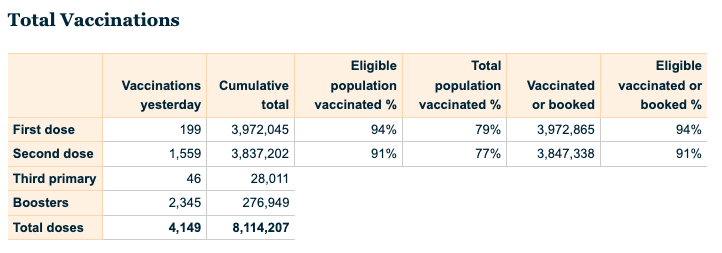
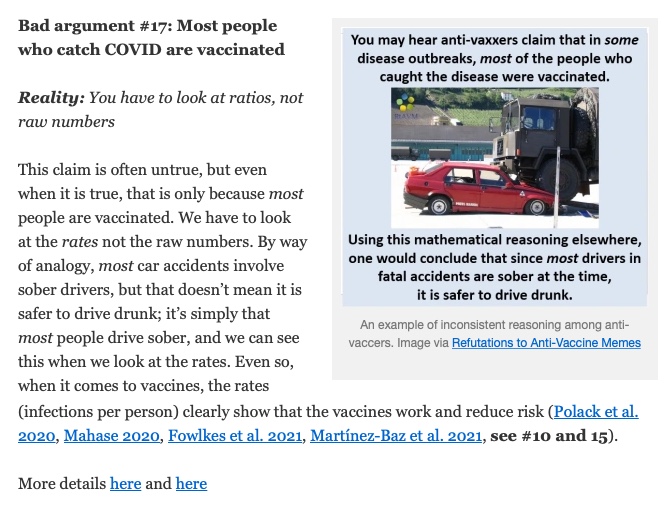
If you don't understand this you don't understand how numbers work. Helpful YouTube videos explaining numbers are available.
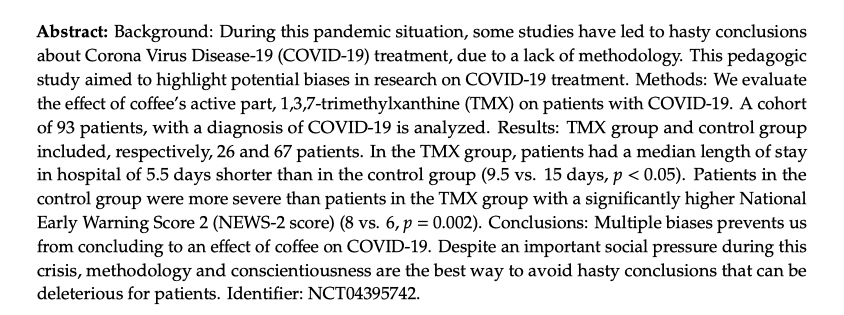
This is kind of the point of science; when the evidence changes so does the recommendation.

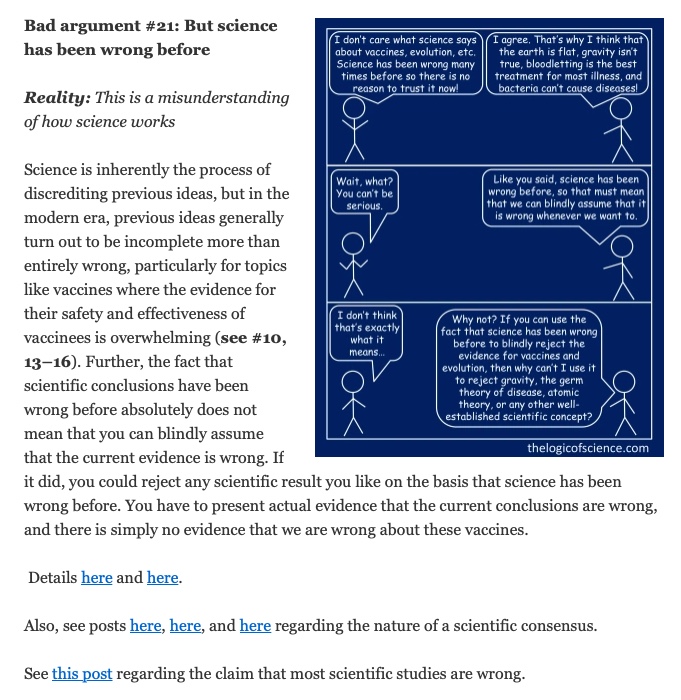
As someone else wrote, they also laughed at Bozo the Clown but it doesn't mean you should take medical advice from him.
This is the weirdest of the non-sequiturs.
For NZ, see CARM: nzphvc.otago.ac.nz/carm/
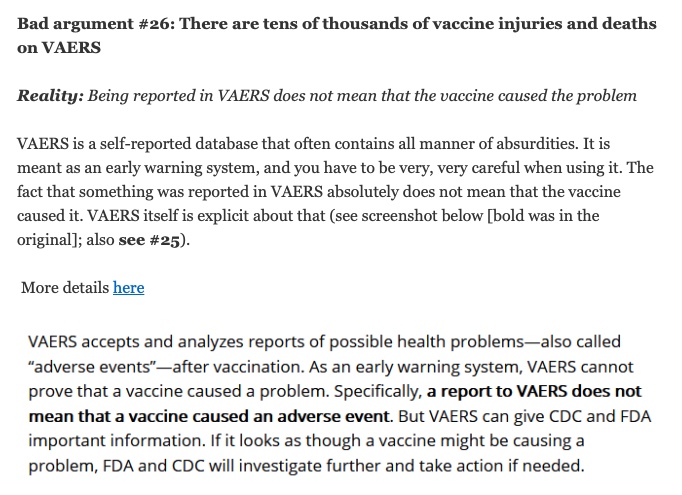
Yes you can self-report your headache & sore arm & would be strongly encouraged to do so. See the bold type below.
Yes you can self-report your headache & sore arm & would be strongly encouraged to do so. See the bold type below.

Thanks for reading. Or blocking me. Either way, I hope some of these are useful. Please visit the site at the top of this thread for the links & the papers that support the arguments being made.
• • •
Missing some Tweet in this thread? You can try to
force a refresh