
Calling all #POCUS fans, and #criticalcare 💓 afficionados! Asking if we have the right tools to identify RV dysfunction (RVD) in ICU?? We took an unbiased view (paper link at end of a long thread 🧵).... 

The RV is not regular and so dysfunction can sometimes be found in one measure but not another - the crooked RV demands more than one guard to be caught playing up! 🇺🇲🇨🇦🇪🇺 consensus cardiology guidelines suggest looking at FAC and TAPSE to define RV systolic dysfunction:

In ICU tho pts are dissimilar to those cardiology sees. Acute pathology with RVD has been variably defined. Acute PE is a useful start; though systolic dysfncn is a prognostic TTE marker RV dilatation and septal behaviour is better recognised. Notably⬆️Troponin --> ⬆️risk too
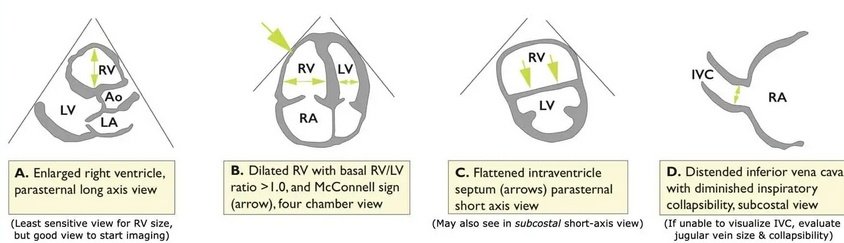
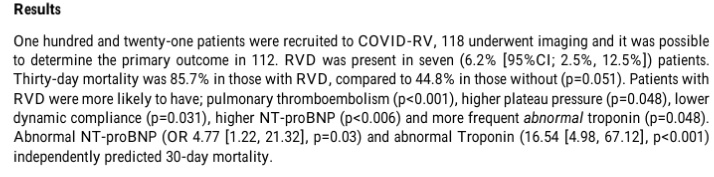
This PE-centric definition of RVD with at least a 1:1 RV:LV ratio was used to define RVD in a recent multi-centre Scottish ICU COVID-19 TTE study; perhaps this is why in >55% of RVD patients a PE was found

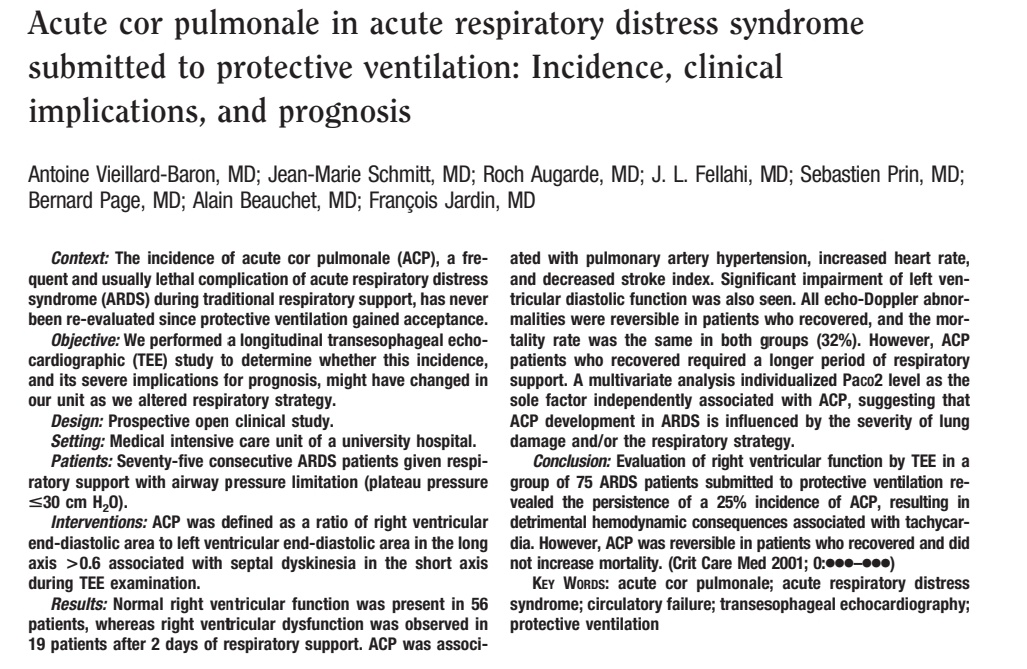
In non-COVID ARDS where RVD is known to commonly occur, it has been defined in a different fashion: a minimum RV:LV ratio of 0.6 with the septum bowing in to embarass the LV cavity - "acute cor pulmonale"
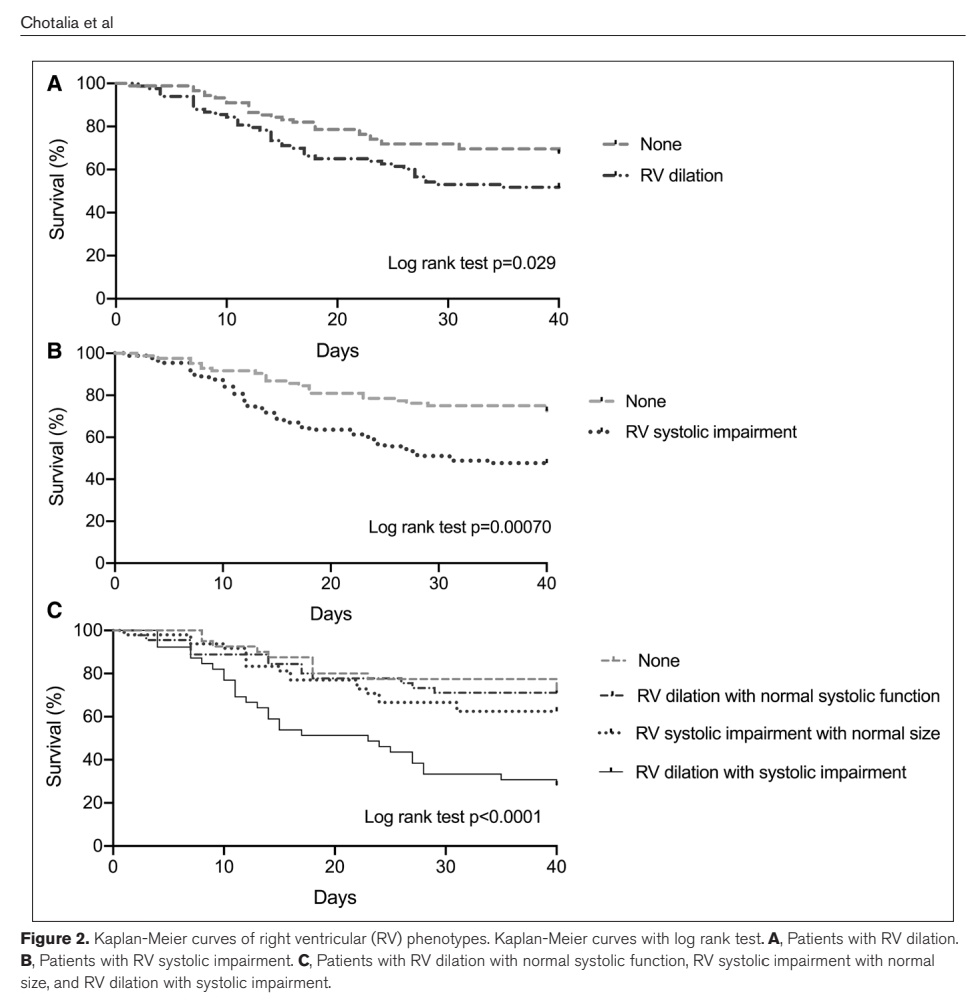
Using different cut-offs & metrics clearly --> different epidemiology of RVD & different outcomes. This is an important problem similar to that seen when comparing studies of renal dysfunctn before KDIGO. So we recently looked at RVD in COVID using systolic & dilatation metrics:
We found that both RVD metrics were associated with mortality but that when both occurred together (dilated + systolic dysfunction) mortality was highest. Our findings contrasted with RVD rates and outcomes in COVID-RV study, highlighting problems with inconsistent definitions
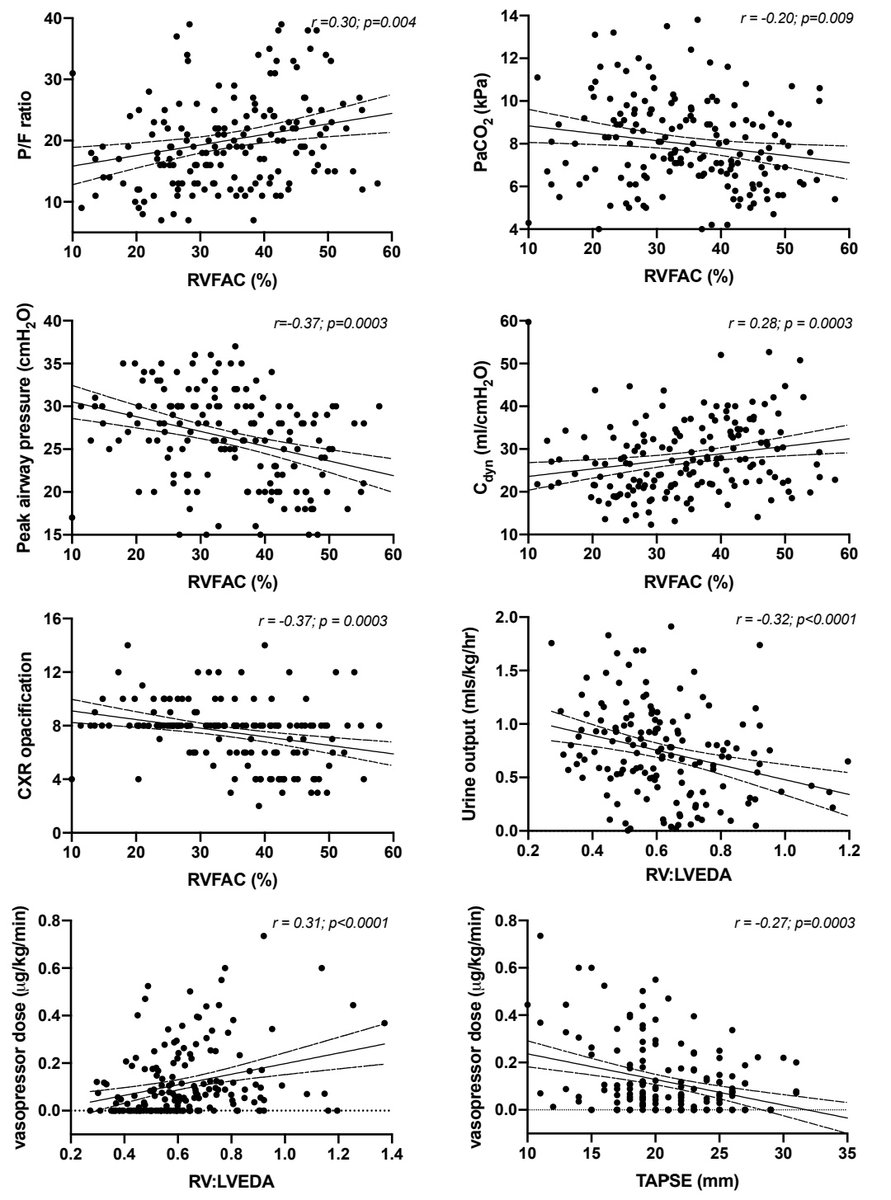
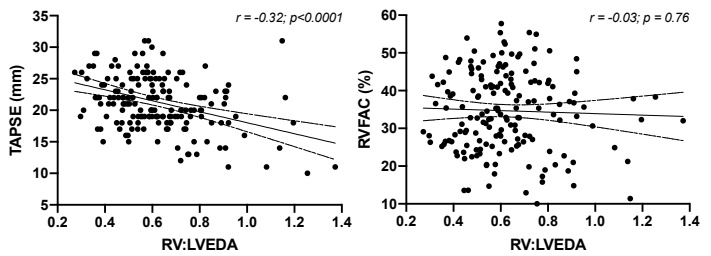
We also found different metrics behaved differently: TAPSE only correlated with vasopressor dose but FAC and dilatation metrics associated with many lung & COVID metrics though not with one another:
We wondered: are there better classifiers that define acute RVD? Are there groups of patients that cluster according to RV behaviour, & can we identify these masked groups? Will we just end up with the same groups we already use???
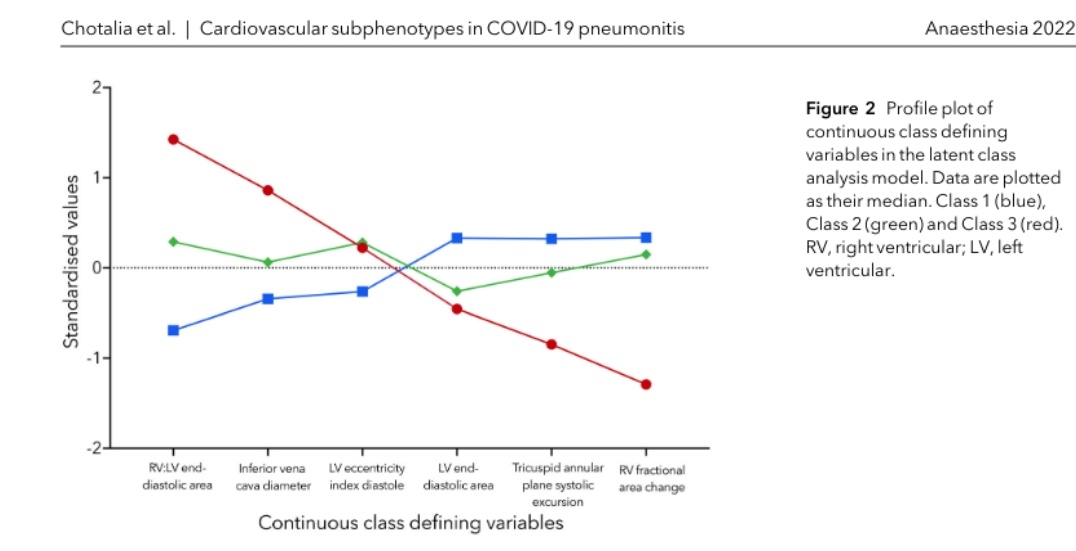
To help answer this qn we turned to latent class analysis and used TTE and haemodynamic variables to see if an unbiased methodology based on
💓 parameters could help better define RVD. LCA identified 3 grps with different relative TTE parameters best fitting as latent classes
💓 parameters could help better define RVD. LCA identified 3 grps with different relative TTE parameters best fitting as latent classes
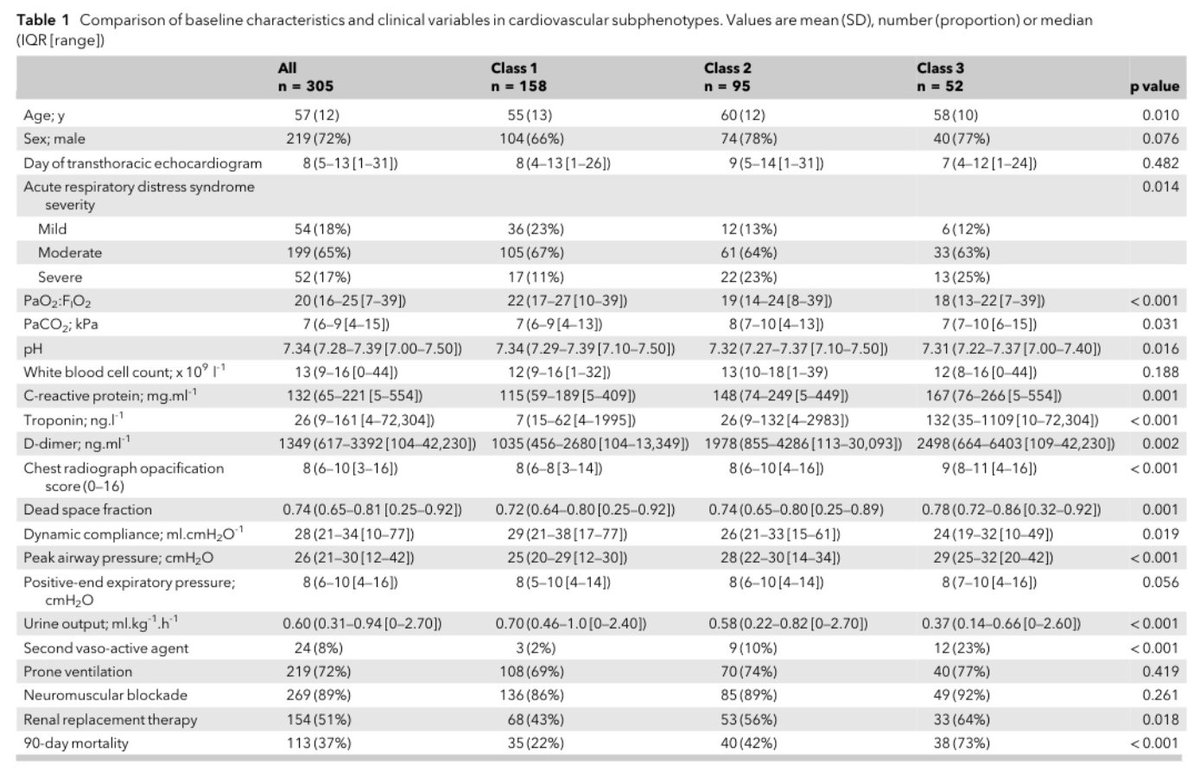
These groups had significantly different clinical characteristics, ventilation parameters & outcomes. Notably, CRP, renal dysfunction and Troponin which weren't used in the LCA data input, featured prominently in class 3, the highest risk group.
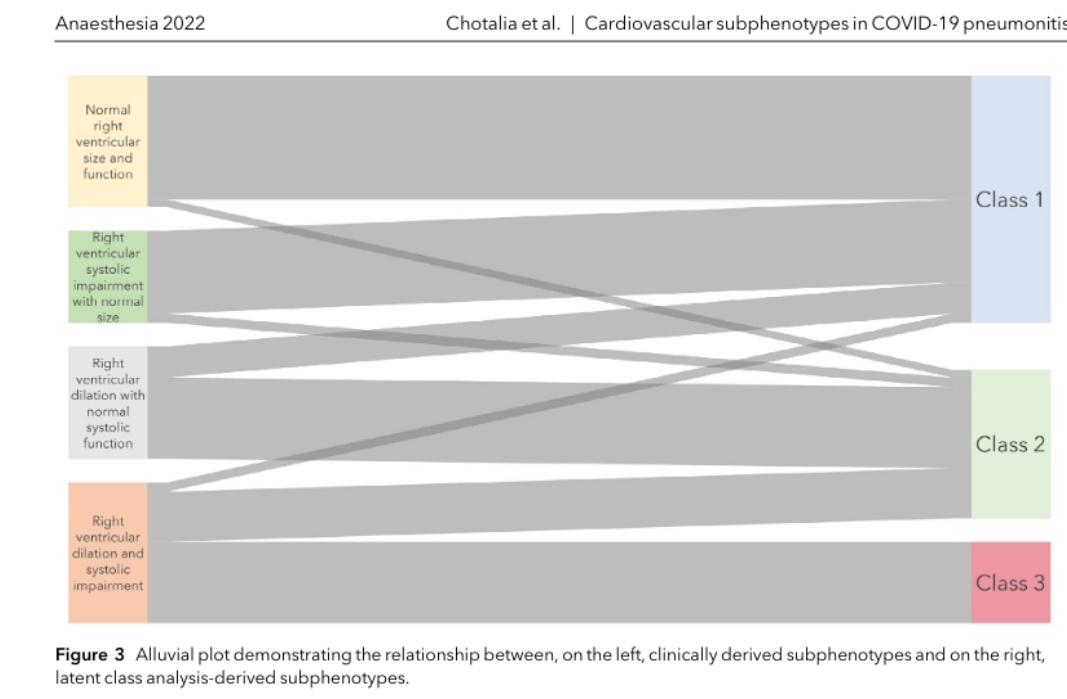
Comparing LCA & usual metrics: crucially, we think LCA shows-up the weakness of current RVD definitions given the crossover we see from each traditional grouping to the LCA classes. Can these groups be used to best risk stratify RVD and lead to trials aimed at protecting the RV??
What more? Well LCA has lately shown consistent bi-clustering in ventilated non-ARDS patients, AKI, ARDS and also COVID-19 when biochemical, inflammatory, haematologic, ventilator & physiologic variables are considered...
Recently pulmonary-centric LCA has also been used to cluster covid patients in two groups with differing outcomes
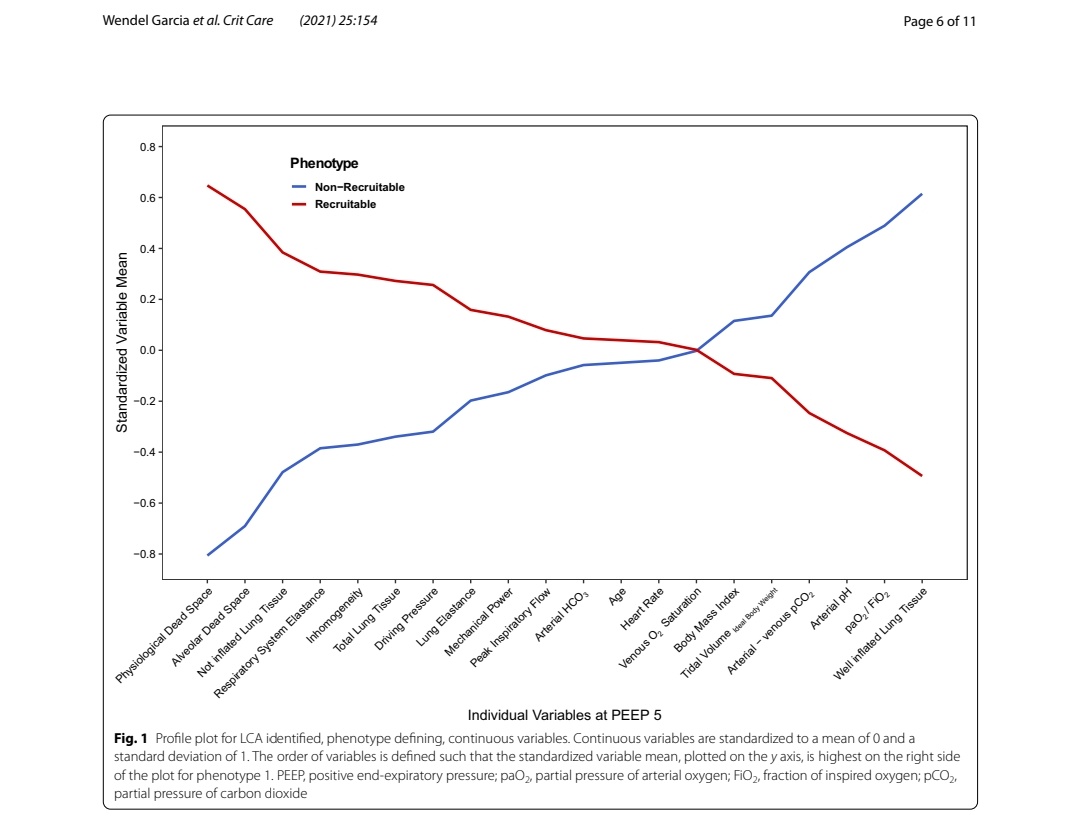
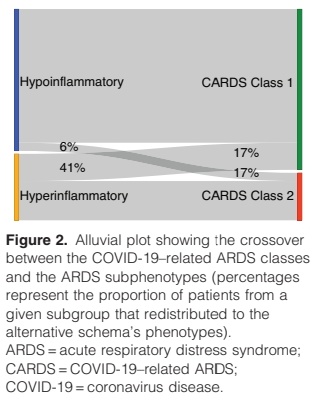
Where does 💓 LCA fit if it generates 3 classes? Our findings of 3 classes must 1st be validated but we noted great overlap between RVD class 3 & CARDS-2. We also think LCA can only produce "images" according to where you put its 👀 - what data you expose it to
It's also unclear that if LCA correctly shows patients cluster in to two phenotypic groups that individual organ function LCA must also cluster in two phenotypes
SUMMARY:
LCA of 💓 parameters identified 3 risk groups of RVD that may better classify RVD in ARDS than current outpatient cardiology metrics. We think this could be an important step in defining RVD to potentially lead to rationale interventions @vaszochios @prorvnet
LCA of 💓 parameters identified 3 risk groups of RVD that may better classify RVD in ARDS than current outpatient cardiology metrics. We think this could be an important step in defining RVD to potentially lead to rationale interventions @vaszochios @prorvnet
Thanks for reading to the end! All credit to our brilliant colleagues & our team: @jaldmn @drjminpat @drdhruvparekh and of course the main man @Mineshc1! Many thanks to @Anaes_Journal for hosting the paper which can be read here: …-publications.onlinelibrary.wiley.com/doi/10.1111/an… @BacrUob @UHBCriticalCare
• • •
Missing some Tweet in this thread? You can try to
force a refresh


