Hot out of press.
"AKI in critically ill patients with cancer"
@ShrutiGkidney @BWHKidney @MGHKidneys @DanaFarber
@kdjhaveri @HofstraKidney
@CJASN
@onconephsociety
@UCincyMedicine @UCKidney @UCincyIM
#Onconephrology
Causes of AKI in pts with cancer in nutshell ⬇️
"AKI in critically ill patients with cancer"
@ShrutiGkidney @BWHKidney @MGHKidneys @DanaFarber
@kdjhaveri @HofstraKidney
@CJASN
@onconephsociety
@UCincyMedicine @UCKidney @UCincyIM
#Onconephrology
Causes of AKI in pts with cancer in nutshell ⬇️

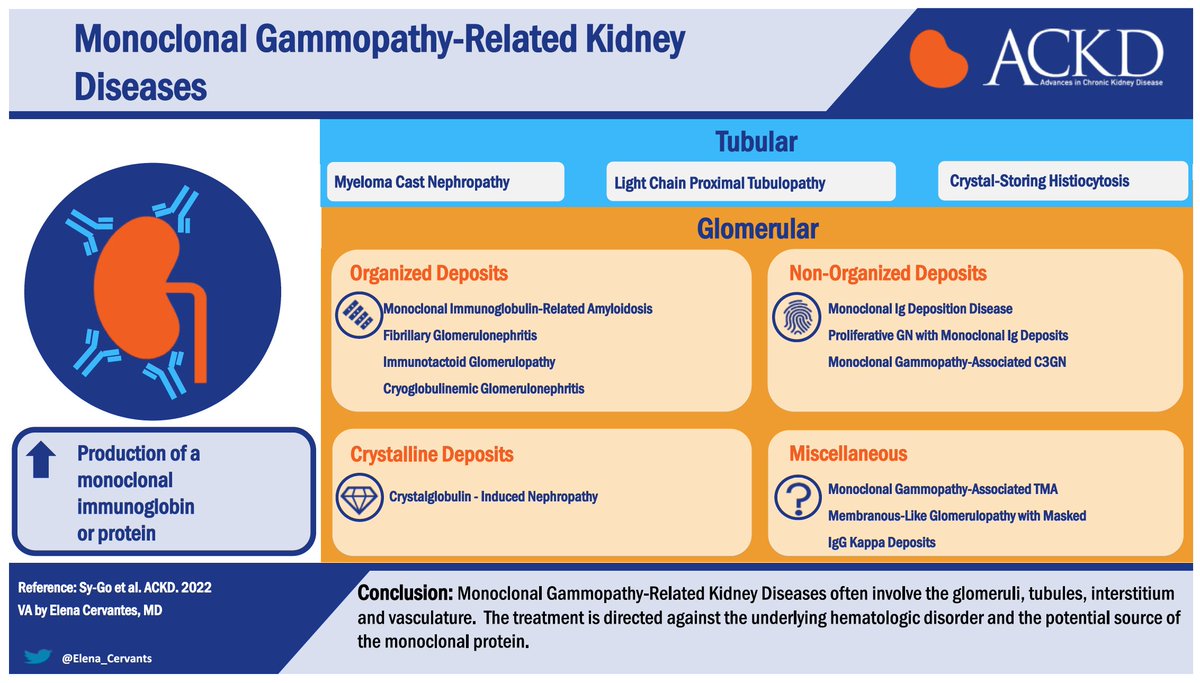
⭐️Phenotypes of AKI from monoclonal gammopathy
⭐️ Data suggest that patients with MGRS are at high risk for progression to kidney failure if not treated with clone-directed therapy (e.g., bortezomib)
Read more about it in the section "Monoclonal Gammopathies and AKI" ⬇️
⭐️ Data suggest that patients with MGRS are at high risk for progression to kidney failure if not treated with clone-directed therapy (e.g., bortezomib)
Read more about it in the section "Monoclonal Gammopathies and AKI" ⬇️

⭐️Other etiologies of AKI in cancer
Hypercalcemia
Direct kidney parenchymal infiltration
Obstruction⬇️
Hypercalcemia
Direct kidney parenchymal infiltration
Obstruction⬇️

⭐️Conventional chemoRx toxicities ⬇️

Prototype chemoRX AKI from Cisplatin : Mediated by apoptosis, inflammation, DNA and mitochondrial injury ⬇️

HSCT associated AKI
The flowchart sums it all ⬇️
The flowchart sums it all ⬇️

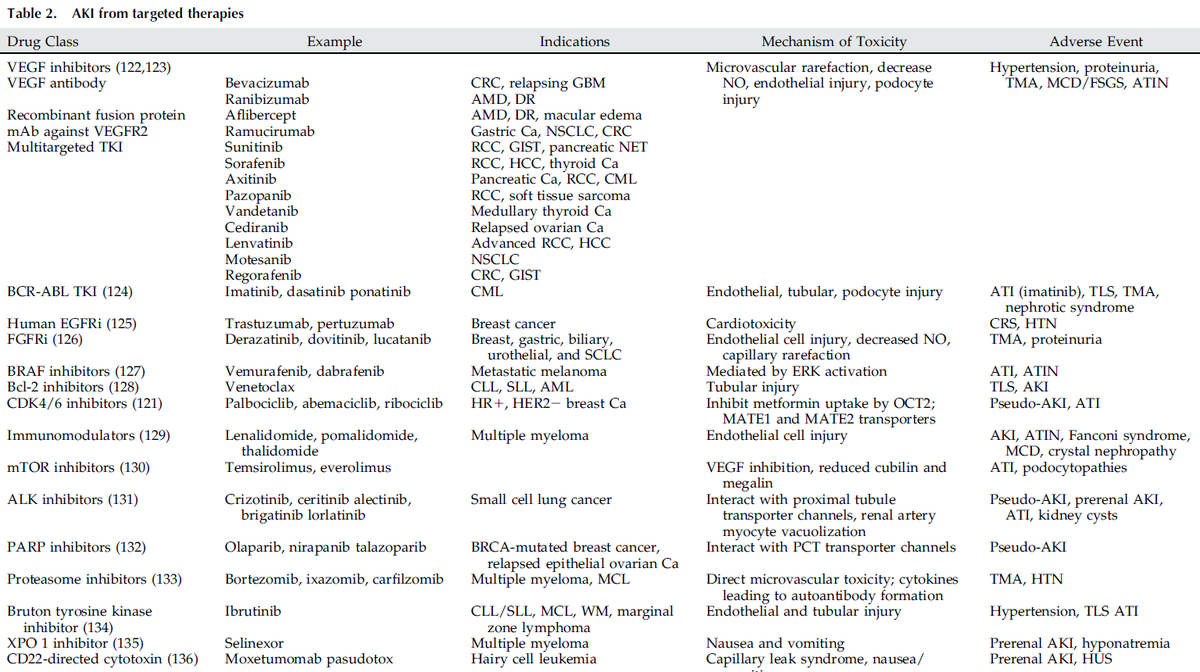
AKI from targeted therapies.
check out the table which summarizes it. ⬇️
check out the table which summarizes it. ⬇️
A brief synopsis of AKI from
-ImmunoRx
-CellularRx (CAR-T cell)
-TMA
-Hemodynamic causes
-TLS⬇️
-ImmunoRx
-CellularRx (CAR-T cell)
-TMA
-Hemodynamic causes
-TLS⬇️

To conclude
⭐️Precision medicine : need to have biomarkers to predict AKI on oncoRx agents
⭐️eg: CRP and urinary retinol binding protein in ICPi-AKI induced AIN
⭐️Can help to identify pseudo-AKI which can happen with drugs like PARP & CDK 4/6 inhibitors
@threadreaderapp
⭐️Precision medicine : need to have biomarkers to predict AKI on oncoRx agents
⭐️eg: CRP and urinary retinol binding protein in ICPi-AKI induced AIN
⭐️Can help to identify pseudo-AKI which can happen with drugs like PARP & CDK 4/6 inhibitors
@threadreaderapp
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh