
1. A 57 yo man is brought to the ED after being assaulted. He was hit in the head with a baseball bat. GCS 7 (E2V2M3), R pupil 6mm and L pupil 3mm, both are reactive to light. CT is obtained. 

2. TBI is a very common reason for admission in the Neuro ICU. In this #NeurocriticalMedEd Tweetorial we’ll cover:
1. Initial presentation & resuscitation
2. Imaging
3. Initial management
4. The battle against ICP
5. Treatment algorithms
6. Other complications
1. Initial presentation & resuscitation
2. Imaging
3. Initial management
4. The battle against ICP
5. Treatment algorithms
6. Other complications
3.1 TBI is commonly classified based on GCS or the FOUR score.
(mild GCS 13-15, moderate GCS 9-12, severe GCS ≤ 8).
FOUR score might have some advantages:
• Better interrater reliability
• Better for intubated patients
• Can recognize different stages of brain herniation
(mild GCS 13-15, moderate GCS 9-12, severe GCS ≤ 8).
FOUR score might have some advantages:
• Better interrater reliability
• Better for intubated patients
• Can recognize different stages of brain herniation
3.2 Find here the GCS and FOUR score references.
pubmed.ncbi.nlm.nih.gov/25030516/
pubmed.ncbi.nlm.nih.gov/16178024/
pubmed.ncbi.nlm.nih.gov/25030516/
pubmed.ncbi.nlm.nih.gov/16178024/
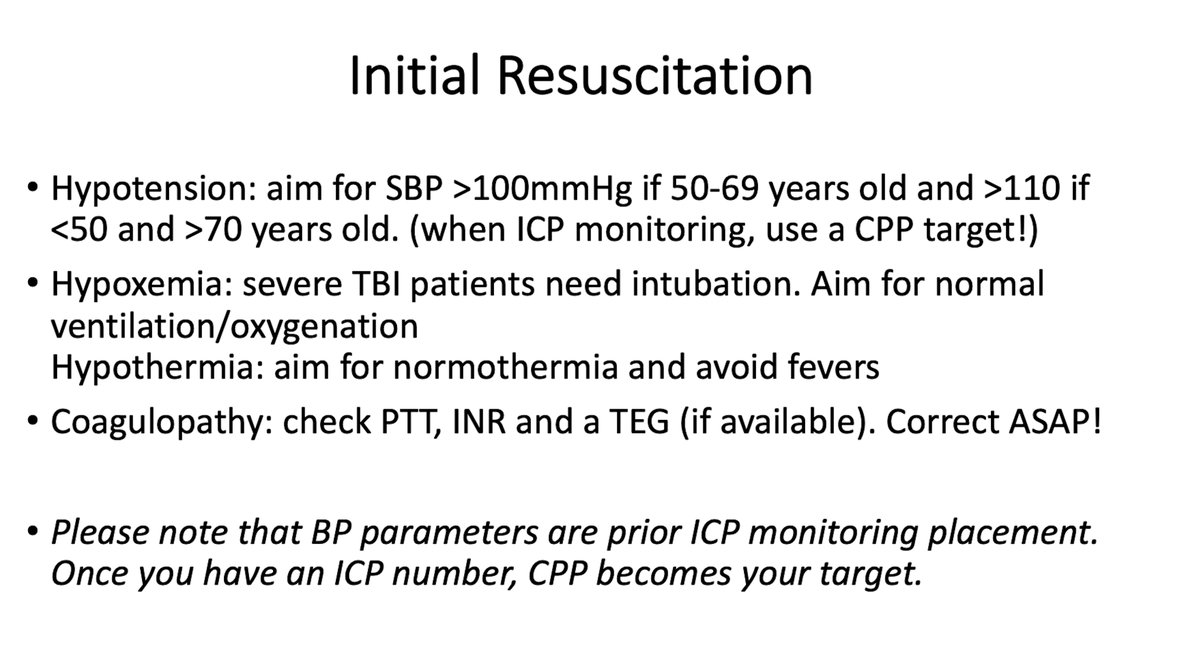
4. Initial resuscitation is very important in TBI.
✴️Hypotension, hypoxemia, hypothermia and coagulopathy are the evils of any trauma
✴️Rapid identification and correction of these factors is critical
✴️C spine stabilizations is a must until it can be cleared
Let’s expand a bit
✴️Hypotension, hypoxemia, hypothermia and coagulopathy are the evils of any trauma
✴️Rapid identification and correction of these factors is critical
✴️C spine stabilizations is a must until it can be cleared
Let’s expand a bit
6. Once stabilized, take your patient to CT. It will guide you to detect lesions, identify treatable ones and guide potential neurosurgical interventions.
Also, several scales are used for description of lesions and prognosis, such as the Marshall scale.
pubmed.ncbi.nlm.nih.gov/16331165/
Also, several scales are used for description of lesions and prognosis, such as the Marshall scale.
pubmed.ncbi.nlm.nih.gov/16331165/

7. Identify who might benefit from surgery early! Common indications for surgery are:
✴️Presence of a subdural hematoma with a thickness >10mm and midline shift >5mm
✴️Presence of an epidural hematoma >30cc
✴️Intraparenchymal hematoma with significant mass effect
✴️Presence of a subdural hematoma with a thickness >10mm and midline shift >5mm
✴️Presence of an epidural hematoma >30cc
✴️Intraparenchymal hematoma with significant mass effect
8. Vascular complications? When possible, get CT and CTA to rule out vascular complications of TBI such as:
✴️Dissections
✴️Pseudoaneurysms
✴️Laceration of vessels
✴️Arterial/venous occlusion
✴️Dissections
✴️Pseudoaneurysms
✴️Laceration of vessels
✴️Arterial/venous occlusion
9. CT is done, patient is being admitted to Neuro ICU, time for optimization!
The following are basic recommendations for basic care of severe TBI patients in the Neuro ICU.
pubmed.ncbi.nlm.nih.gov/28187802/
Picture obtained from the SIBICC protocol 👇👇
The following are basic recommendations for basic care of severe TBI patients in the Neuro ICU.
pubmed.ncbi.nlm.nih.gov/28187802/
Picture obtained from the SIBICC protocol 👇👇

10.1 What about tranexamic acid?
CRASH-3 trial showed↓head-injury related mortality in mild-mod TBI with bleeding if TXA is given within 3 hours from trauma. However, this remains very controversial and it’s not universally given.
CRASH-3 trial showed↓head-injury related mortality in mild-mod TBI with bleeding if TXA is given within 3 hours from trauma. However, this remains very controversial and it’s not universally given.

10.2 Another recent study found prehospital TXA associated with increased mortality in pts with isolated severe TBI.

11. When to repeat CT?

12. Before moving on, we strongly recommend reviewing our first Tweetorial about ICP to review basic concepts and rationale for treatment!
https://twitter.com/NeurocriticalE/status/1420930470938910721
13. Our patient had an EVD placed. You are called for an ICP of 30mmHg. The ICP battle starts!
With the objective of addressing efficacy, sequential order or combination of treatments against elevated ICP, the SIBICC algorithm was proposed.
pubmed.ncbi.nlm.nih.gov/31659383/
With the objective of addressing efficacy, sequential order or combination of treatments against elevated ICP, the SIBICC algorithm was proposed.
pubmed.ncbi.nlm.nih.gov/31659383/

14.1 What if we have a patient with no ICP monitor?
The BEST:TRIP trial:
✴️Care focused on mantaining monitored ICP<20 was not superior to care based on imaging and clinical examination.
pubmed.ncbi.nlm.nih.gov/23234472/
The BEST:TRIP trial:
✴️Care focused on mantaining monitored ICP<20 was not superior to care based on imaging and clinical examination.
pubmed.ncbi.nlm.nih.gov/23234472/
14.2 The Consensus-Based Management Protocol (CREVICE) for the treatment of severe TBI based on imaging and clinical examination alone addressed this. Check out the algorithm!
The CREVICE protocol is derived from the BEST:TRIP trial.
pubmed.ncbi.nlm.nih.gov/32013721/
The CREVICE protocol is derived from the BEST:TRIP trial.
pubmed.ncbi.nlm.nih.gov/32013721/
15. What about 2dary decompressive craniectomy (DC) for refractory ICP (to contrast with primary DC intended to evacuate lesions such as hematomas)?

16.1 Some other factors
✴️Feed your patients. Meeting calorie requirement by the 5th day 👇 mortality.
✴️Steroids associated with ↑ mortality in severe TBI
✴️Hypothermia has not been shown to improve outcomes
✴️Feed your patients. Meeting calorie requirement by the 5th day 👇 mortality.
✴️Steroids associated with ↑ mortality in severe TBI
✴️Hypothermia has not been shown to improve outcomes
16.2 ....
✴️There is no evidence to suggest timing of starting DVT prophylaxis. Consider starting it if bleed has been stable for 24-48h.
tinyurl.com/4h5mzank
✴️There is no evidence to suggest timing of starting DVT prophylaxis. Consider starting it if bleed has been stable for 24-48h.
tinyurl.com/4h5mzank
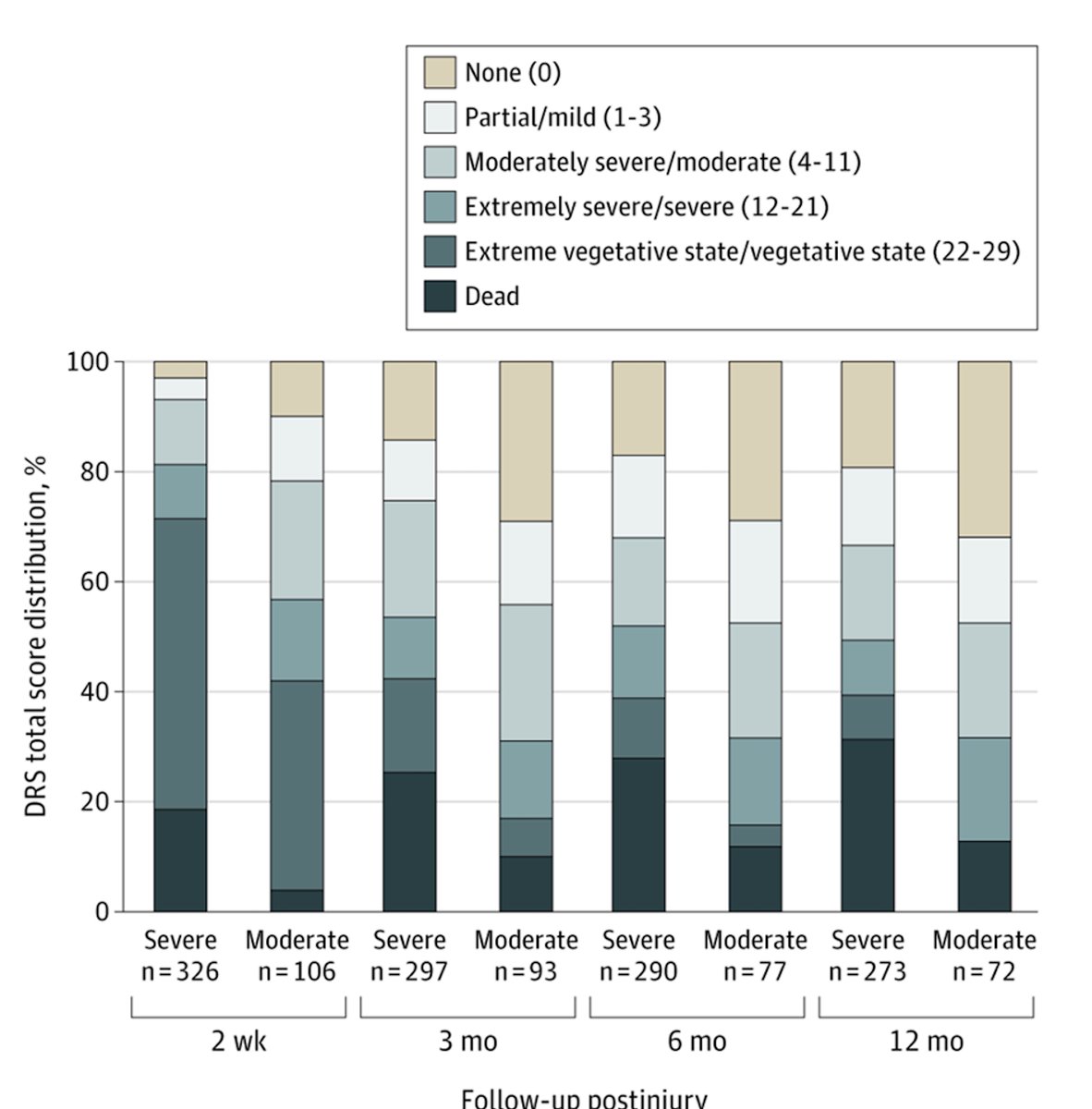
17.1 Prognosis? The most relevant prognostic model is IMPACT 👉 age, Glasgow motor score, pupillary reactivity and the presence of subarachnoid hemorrhage are the most important prognostic factors.
pubmed.ncbi.nlm.nih.gov/18684008/
pubmed.ncbi.nlm.nih.gov/18684008/

17.2 Important!!
Major functional gains, including recovery of independence, can be achieved up to 12 months postinjury.
pubmed.ncbi.nlm.nih.gov/34228047/
Major functional gains, including recovery of independence, can be achieved up to 12 months postinjury.
pubmed.ncbi.nlm.nih.gov/34228047/
18. Multimodal monitoring? Partial brain tissue oxygenation (PbtO2)?
The BOOST II trial assessed management of TBI based on ICP alone vs ICP + PbtO2. The intervention group demonstrated a trend towards lower mortality and favorable outcomes.
The BOOST II trial assessed management of TBI based on ICP alone vs ICP + PbtO2. The intervention group demonstrated a trend towards lower mortality and favorable outcomes.


19. Let’s wrap up! In a case of difficult to control ICP, based on the SIBICC protocol, which of the following represents a tier 3 treatment strategy?
20. Next week we'll have 2 tweetorials. See you on Tuesday!
• • •
Missing some Tweet in this thread? You can try to
force a refresh



