
Ok folks, pay attention. Percent lifespan extension means nothing when the controls are short-lived. The next time someone Tweets about how “X increases lifespan in mice by Y percent!!!”, first thing you should do is look at the absolute lifespan of the controls /1
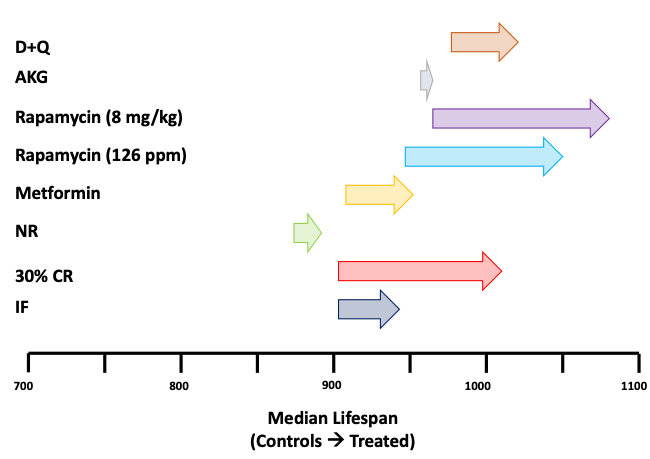
Short-lived controls are a major source of false-positive results in mouse lifespan studies. Metformin, nicotinamide riboside, intermittent fasting all suffer from this flaw. This graphic illustrates the problem /2 

Left side of arrows indicate median LS of the control group, right side indicates median LS of treatment group for different interventions. All male C57BL/6 mice. Closest apples to apples as I could come.
Further explanation here starting at ~6:25:
/3
Further explanation here starting at ~6:25:
/3
You will note that for several of the “long-lived” intervention groups, their median lifespan is shorter than the control groups in other studies. In other words, the "long-lived" intervention groups would have been short-lived in those experiments /4
Perhaps related, those interventions with short-lived controls like metformin and nicotinamide riboside are also the ones that did not reproduce as long-lived when tested by the ITP.
***Short-lived controls give rise to false positives***
/5
***Short-lived controls give rise to false positives***
/5
For the diet gurus out there, this contributes to my lack of confidence that intermittent fasting/time restricted feeding is going to reproducibly extend lifespan when calorically matched to controls /6
You all know I'm bullish about rapamycin. Just look at the rapamycin absolute effect compared to the others and you’ll understand why. I like interventions that work well, and work every time. Show me something better and I’ll get on board /7
Someone will undoubtedly complain that this isn’t a fair comparison because some studies, like the senolytic study, started treatment late in life. So to control for this, I redid the analysis excluding all deaths prior to 820 days, and the effect is even more pronounced /8
This was all done with median lifespan using this tool to approximate the raw data, since almost nobody actually provides that in their papers: automeris.io/WebPlotDigitiz…
/9
/9
Data from these studies:
Rapamycin: eLife 5:e16351. 2016
Metformin: Nat Commun 4, 2192. 2013
D+Q: Nat Med. 24, 1246-1256. 2018
IF and CR: Cell Metab 221-228. 2019
AKG: Cell Metab 32, 447-456. 2020
NR: Science 352, 1436-1443. 2016
/10
Rapamycin: eLife 5:e16351. 2016
Metformin: Nat Commun 4, 2192. 2013
D+Q: Nat Med. 24, 1246-1256. 2018
IF and CR: Cell Metab 221-228. 2019
AKG: Cell Metab 32, 447-456. 2020
NR: Science 352, 1436-1443. 2016
/10
I also like maximum lifespan as a metric to evaluate interventions. In male mice treated for 3 months with 8 mg/kg/d rapamycin, ~20% lived past 1200 days and the longest-lived mouse > 1400 days. If shiny new drug X doesn’t at least do this well, why should we get excited?
/11
/11
Here’s an egregious example of the short-lived control with the truly remarkable claim *in the abstract* that “the residual lifespan of the naturally aged mice was extended by 80%”. Unfortunately, this all falls apart when you look at the actual data
onlinelibrary.wiley.com/doi/10.1111/ac…
/12
onlinelibrary.wiley.com/doi/10.1111/ac…
/12
Here is the survival curve from that study. Note that the control median is about 620d, the “long-lived” berberine group ~710d.
This is C57BL/6 males, same as our 2016 eLife study, where the controls were ~900d and the rapamycin treated were ~1050d /13
This is C57BL/6 males, same as our 2016 eLife study, where the controls were ~900d and the rapamycin treated were ~1050d /13

And here is berberine added to the prior graphic. You can see the control is dramatically shorter-lived than even the short-lived controls for metformin, NR, and IF. Berberine might actually increase lifespan, but my guess is not /14

There are a lot of resources being put toward studying things with incremental or zero effects on aging. We only get so many shots on goal. IMO, we should be paying ore attention to things that actually work reproducibly and robustly /15
The message here is simple. Don’t be fooled by the spin and hype. Read past the abstract and actually look at the data. 16/16
• • •
Missing some Tweet in this thread? You can try to
force a refresh




