
Here’s a fun ICU riddle - why do these two different patients both have funny colored effluent in their CRRT bags?
#FOAMed #FOAMcc
1/
#FOAMed #FOAMcc
1/
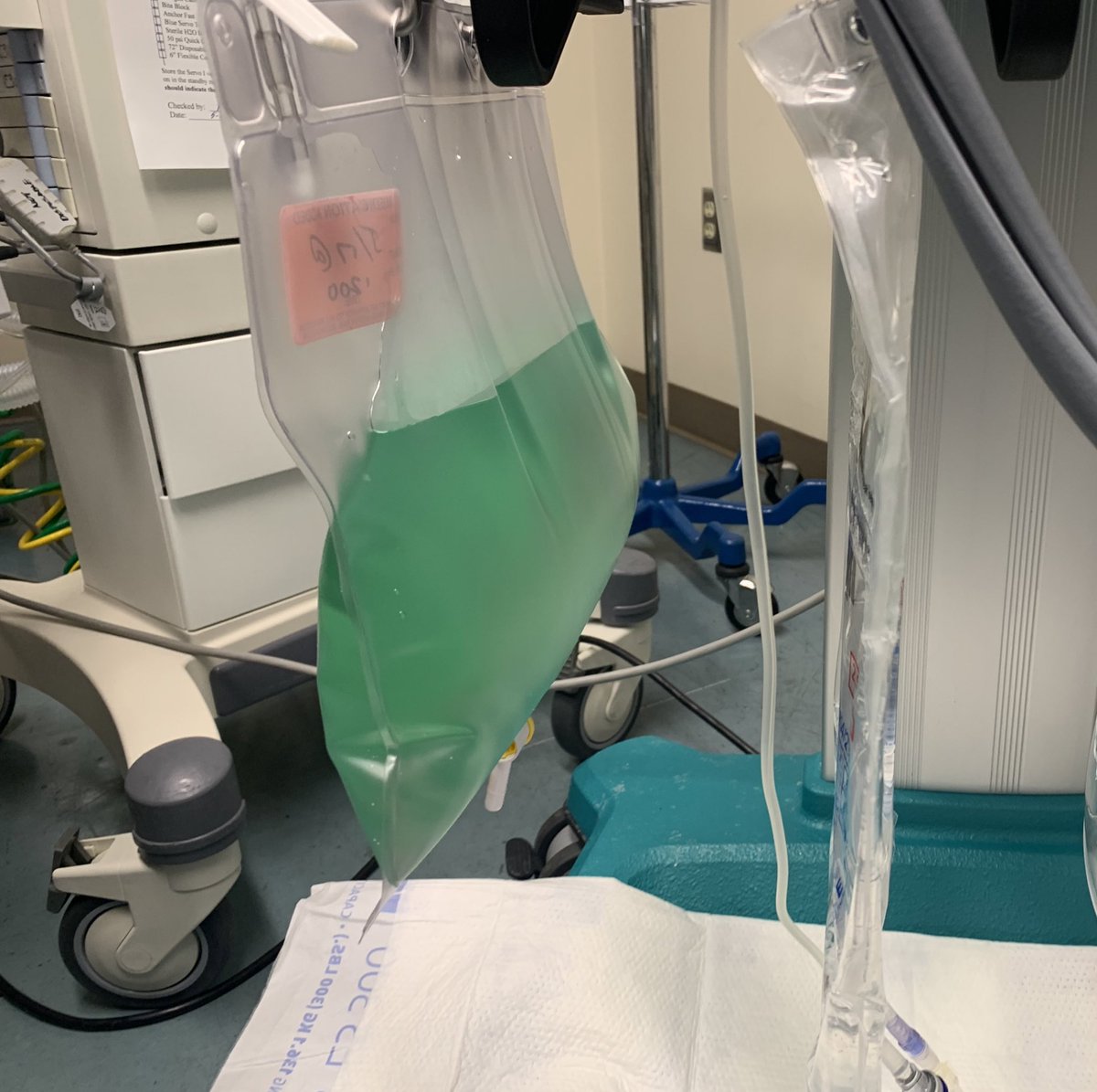

One patient received methylene blue (causing green urine & effluent) and the other received hydroxycobalamin (causing dark red urine & effluent).
But what do these two cases have in common?
2/
But what do these two cases have in common?
2/




The explanation is that both of these patients had vasopressor refractory shock.
Both methylene blue and hydrocobalamin can be used for refractory distributive shock.
Methylene blue
ncbi.nlm.nih.gov/pmc/articles/P…
Hydroxycobalamin
ncbi.nlm.nih.gov/pmc/articles/P…
But why?
3/
Both methylene blue and hydrocobalamin can be used for refractory distributive shock.
Methylene blue
ncbi.nlm.nih.gov/pmc/articles/P…
Hydroxycobalamin
ncbi.nlm.nih.gov/pmc/articles/P…
But why?
3/
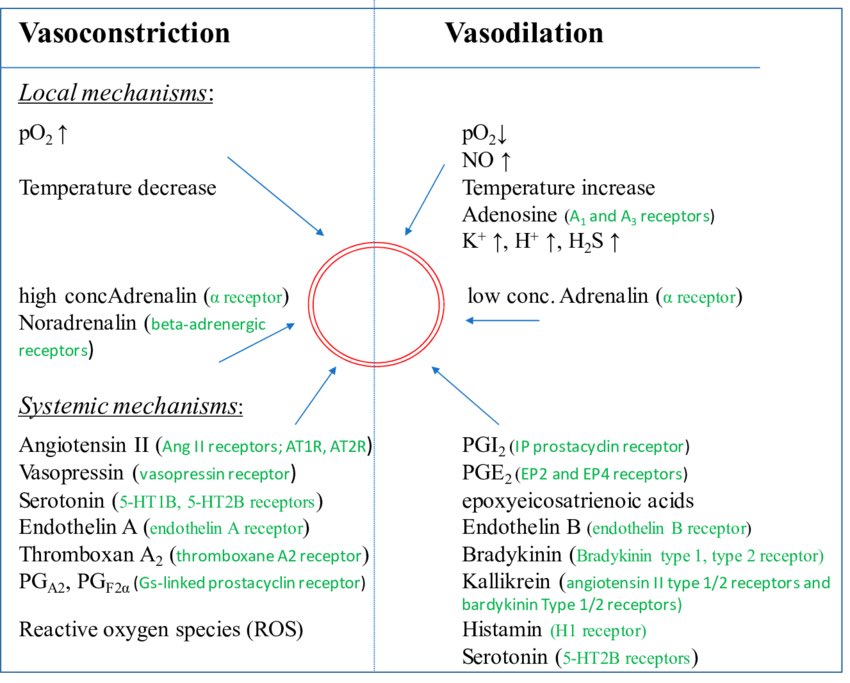
Blood pressure (MAP) is determined by cardiac output (CO) & vascular tone (SVR).
Vascular tone (how much the arteriolar smooth muscle is squeezing) is determined by the balance of endogenous vasoconstrictors (epi, norepi, etc) & vasodilators (Nitric oxide, hydrogen sulfide).
4/
Vascular tone (how much the arteriolar smooth muscle is squeezing) is determined by the balance of endogenous vasoconstrictors (epi, norepi, etc) & vasodilators (Nitric oxide, hydrogen sulfide).
4/
As an analogy, imagine a bad 🚗 driver with one foot continuously on the brake & one on the gas.
The speed of the car (SVR) will be determined by the balance of pressure on the gas (vasoconstriction) & the brake (vasodilation).
5/
The speed of the car (SVR) will be determined by the balance of pressure on the gas (vasoconstriction) & the brake (vasodilation).
5/

Usually to make the 🚗 go faster (treat distributive shock) we press harder on the gas (by adding vasopressors). But sometimes the better approach is to take the foot off the brake pedal (by removing vasodilators).
This is where methylene blue & hydroxycobalamin come in!
6/
This is where methylene blue & hydroxycobalamin come in!
6/
In some shock states there may be a vasodilator excess:
Exposure to a membrane lung during bypass surgery leads to excessive NO & H₂S release
ncbi.nlm.nih.gov/pmc/articles/P…
In severe liver disease, NO & H₂S accumulate because they aren’t being metabolized
ncbi.nlm.nih.gov/pmc/articles/P…
7/
Exposure to a membrane lung during bypass surgery leads to excessive NO & H₂S release
ncbi.nlm.nih.gov/pmc/articles/P…
In severe liver disease, NO & H₂S accumulate because they aren’t being metabolized
ncbi.nlm.nih.gov/pmc/articles/P…
7/
In situations of vasodilator excess, a strategy of “scavenging vasodilators” can be very effective.
Another situation where “vasodilator scavenging” is useful is when conventional vasopressors are rendered ineffective, such as in a beta blocker overdose.
8/
Another situation where “vasodilator scavenging” is useful is when conventional vasopressors are rendered ineffective, such as in a beta blocker overdose.
8/
Methylene blue & hydroxycobalamin are useful adjuncts when pressors aren’t working but they aren’t good *first line* treatments for a few reasons:
First, anaphylaxis to methylene blue is rare but happens. (Anaphylaxis to vasopressors is very unlikely)
pubmed.ncbi.nlm.nih.gov/33055586/
9/
First, anaphylaxis to methylene blue is rare but happens. (Anaphylaxis to vasopressors is very unlikely)
pubmed.ncbi.nlm.nih.gov/33055586/
9/
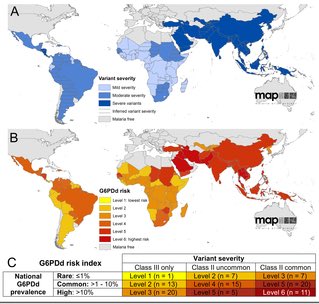
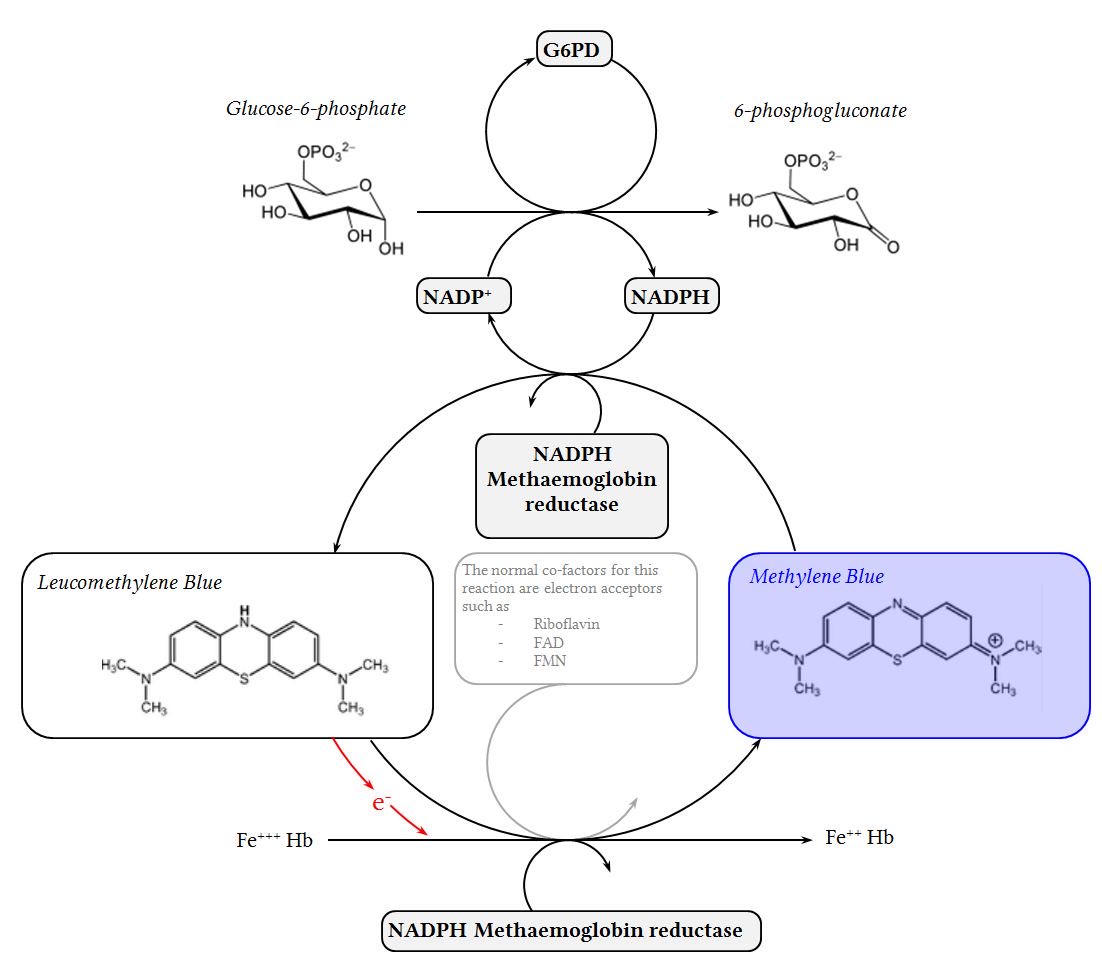
Methylene blue requires an enzyme called glucose 6 phosphate dehydrogenase (G6PD) in order to work. G6PD deficiency (G6PDD) is the most common enzyme deficiency in the world (about 8% of people, more in Africa & Asia).
Methylene blue can cause hemolysis in people with G6PDD.
10/
Methylene blue can cause hemolysis in people with G6PDD.
10/
Second, neither of these drugs is immediately available:
Pharmacy has to mix methylene blue by patient weight. Hydroxycobalamin isn’t stored in the unit.
In a time sensitive emergency (like a hypotensive patient) I’m always going to hang or push other vasopressors first.
11/
Pharmacy has to mix methylene blue by patient weight. Hydroxycobalamin isn’t stored in the unit.
In a time sensitive emergency (like a hypotensive patient) I’m always going to hang or push other vasopressors first.
11/
Finally, as we noted at the top, both of these drugs are brightly colored. This can interfere with a number of tests & equipment.
For example, Methylene blue can interfere with pulse ox readings, causing a spurious low reading. pubmed.ncbi.nlm.nih.gov/3681358/
12/
For example, Methylene blue can interfere with pulse ox readings, causing a spurious low reading. pubmed.ncbi.nlm.nih.gov/3681358/
12/
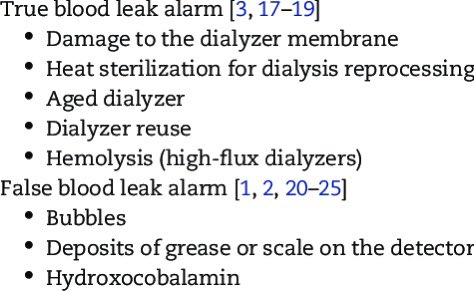
Hydroxycobalamin also causes some problems in patients on intermittent hemodialysis.
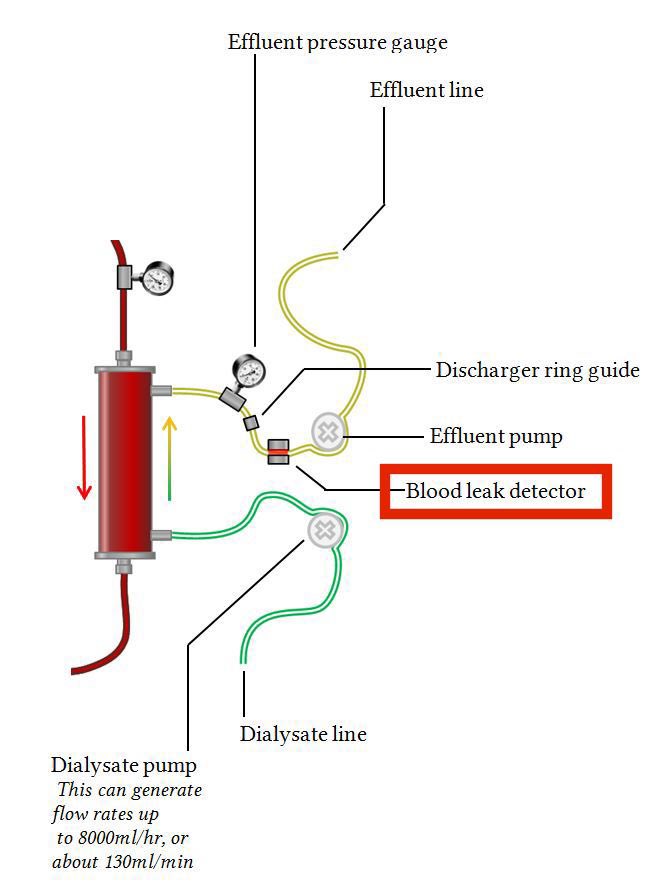
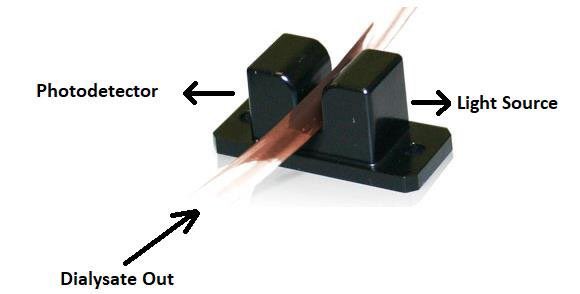
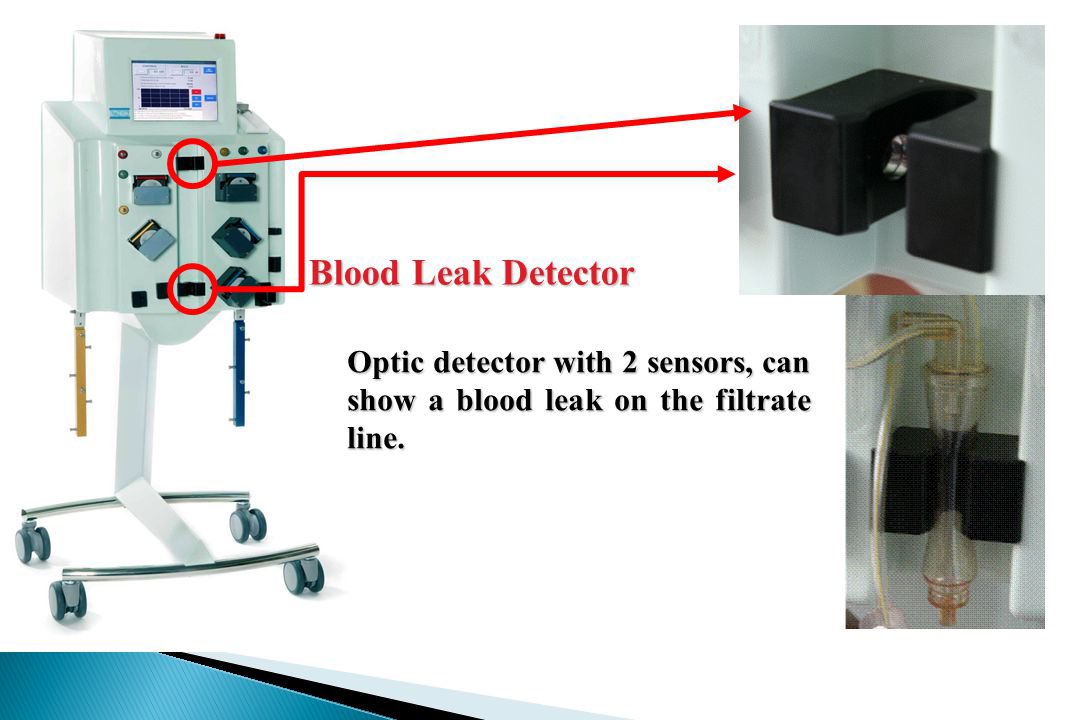
HD machines have a sensor to detect if blood is leaking out of the dialyzer into the effluent.
Because of its red color, hydroxycobalamin makes this sensor alarm.
pubmed.ncbi.nlm.nih.gov/31701774/
13/
HD machines have a sensor to detect if blood is leaking out of the dialyzer into the effluent.
Because of its red color, hydroxycobalamin makes this sensor alarm.
pubmed.ncbi.nlm.nih.gov/31701774/
13/
To summarize:
- we can treat distributive shock either by adding vasopressors or by scavenging vasodilators with methylene blue & hydroxocobalamin
- both of these therapies can have dramatic results in “vasopressor refractory” patients but they have important side effects too
14/
- we can treat distributive shock either by adding vasopressors or by scavenging vasodilators with methylene blue & hydroxocobalamin
- both of these therapies can have dramatic results in “vasopressor refractory” patients but they have important side effects too
14/
https://twitter.com/nickmmark/status/1484774717189869568
Let’s conclude by testing what you learned in this #tweetorial:
1. Methylene blue can be used to treat refractory distributive shock, however it can have important side effects.
Side effects of methylene blue include all of the following EXCEPT:
1. Methylene blue can be used to treat refractory distributive shock, however it can have important side effects.
Side effects of methylene blue include all of the following EXCEPT:
• • •
Missing some Tweet in this thread? You can try to
force a refresh































