Slipped into the Optimizing antihypertensives medications selection in hemodialysis patients with Jennifer Flythe. #NKFClinicals

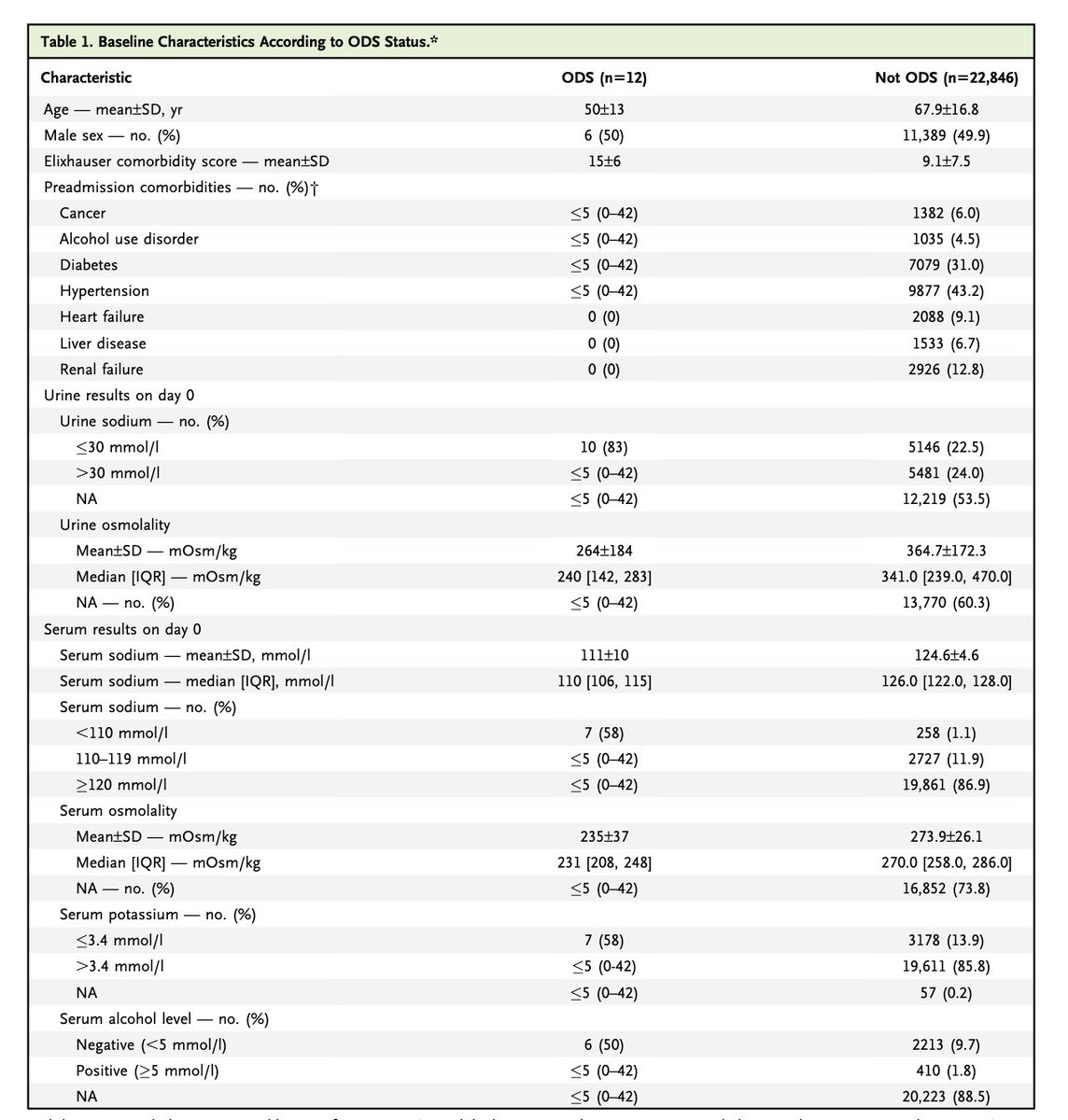
Treating blood pressure in HD reduces outcomes (just barely) #NKFClinicals 
But we have no idea how low to go and we know that treating BP increases dialysis complications (cramps, nausea, hypotension) #NKFClinicals


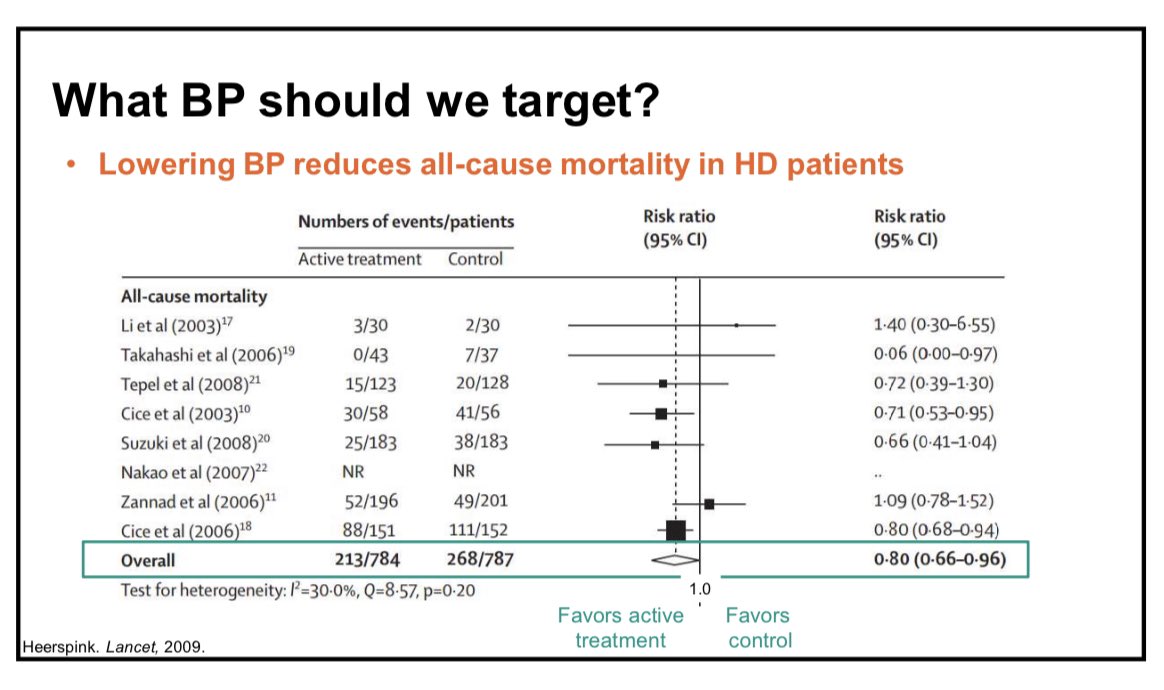
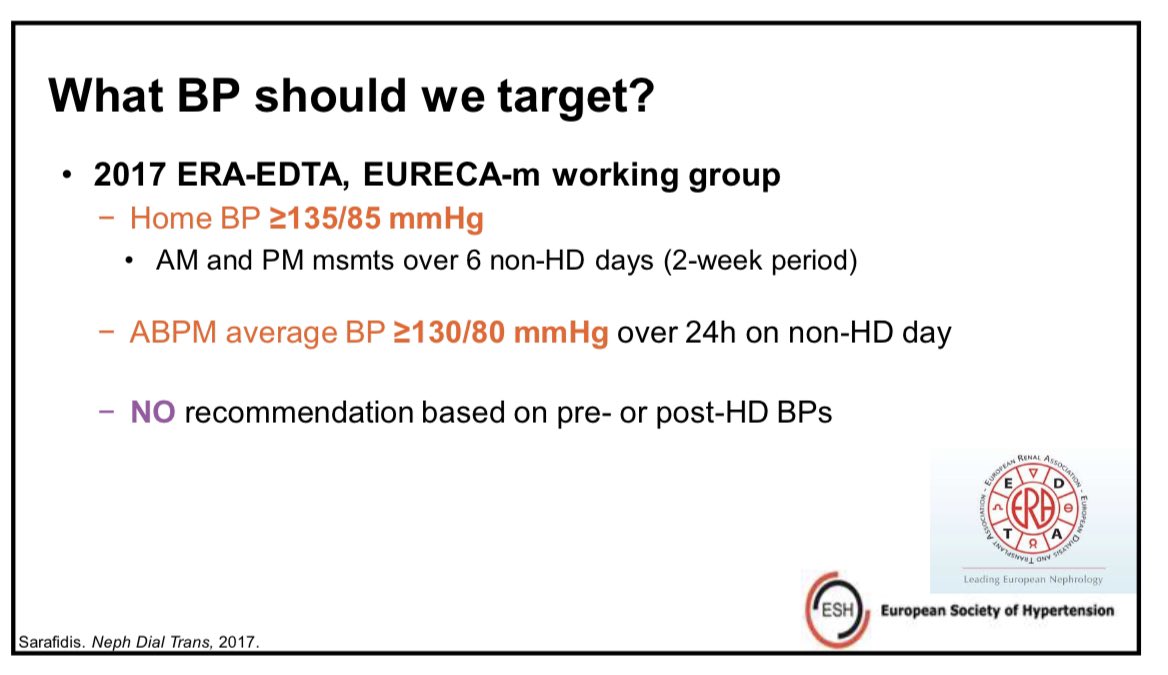
Here are guidelines from Europe. No data to support these guidelines. Do not use on treatment blood pressures. #NKFClinicals
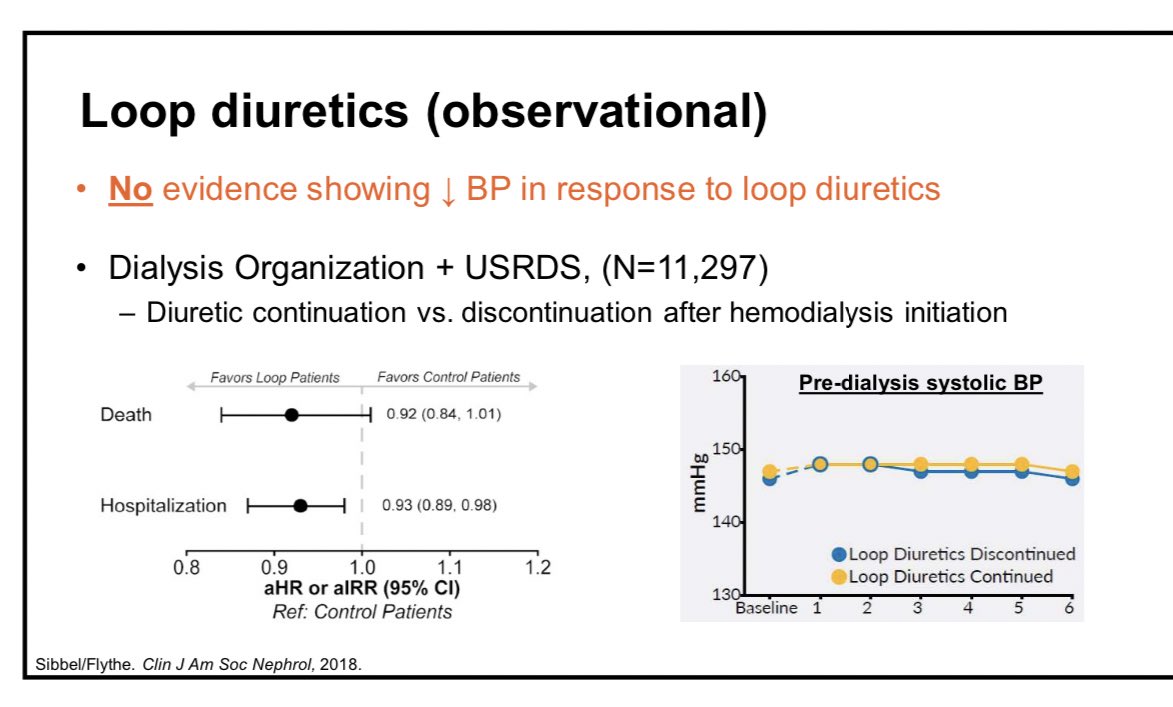
No evidence that loop diuretics lower blood pressure in dialysis patients but remaining on loop after starting dialysis reduced hospitalizations and nearly reduced death. #ObservationalData #NKFClinicals #NKFClinicals
ARCADIA trial from Italy. ACE/ARB vs non-RASi therapy. No difference in composite CV, Death, MI, stroke. No difference in BP #NKFClinicals

Now HDPAL Trial:
Atenolol more BOP lowering than lisinopril. Improved outcomes in atenolol compared to lisinopril. #NKFClinicals
Atenolol more BOP lowering than lisinopril. Improved outcomes in atenolol compared to lisinopril. #NKFClinicals
ARCADIA vs HDPAL
She suggests that race differences may explain differences in outcomes between Italy and Indiana. #NKFClinicals
She suggests that race differences may explain differences in outcomes between Italy and Indiana. #NKFClinicals

CCB
She argues, convincingly, that we should be looking at these drugs vs active controls rather than placebos. #NKFClinicals
She argues, convincingly, that we should be looking at these drugs vs active controls rather than placebos. #NKFClinicals

Interesting and impressive spironolactone data #NKFClinicals

Dialyzability of common anti-hypertensives
She is concerned about the routine holding of blood pressure medications on dialysis days. #NKFClinicals
She is concerned about the routine holding of blood pressure medications on dialysis days. #NKFClinicals

Interesting: @taraichang did a cluster RCT of holding anti hypertensive meds on dialysis days. Taking BP meds was non-inferior to holding antihypertensives. #NKFClinicals
What she does and recommends
Home blood pressure
Treat if interdialytic hypertension > 150 mmHg and avoids it is interdialytic SBP < 120.
#NKFClinicals
Home blood pressure
Treat if interdialytic hypertension > 150 mmHg and avoids it is interdialytic SBP < 120.
#NKFClinicals
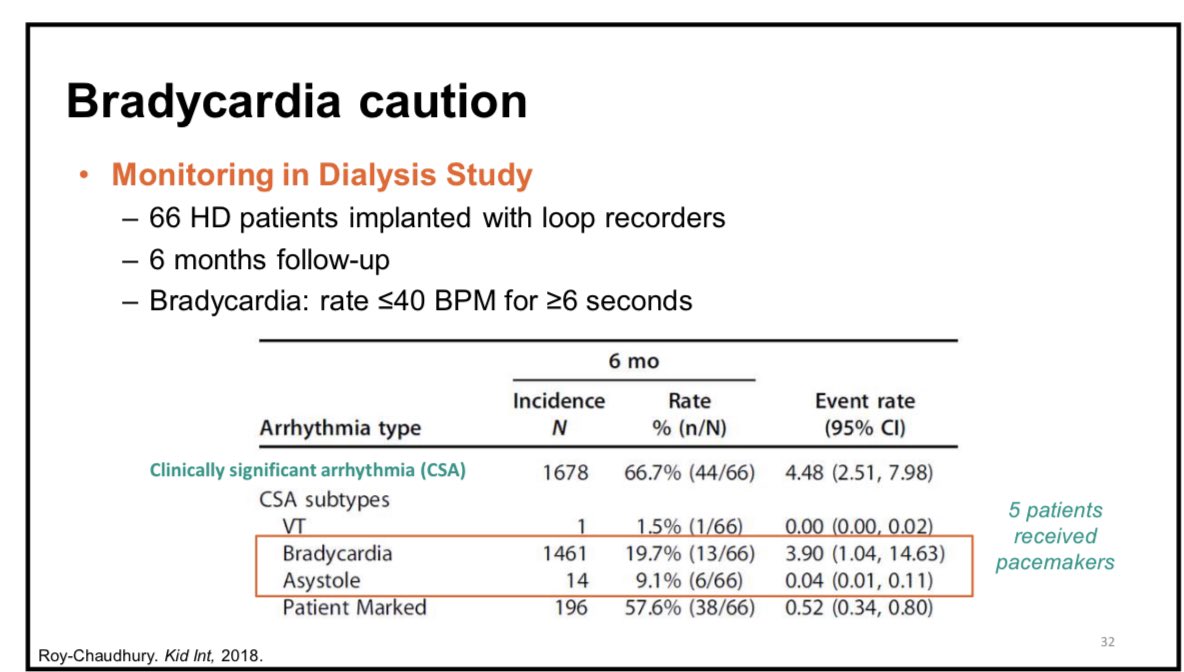
Despite the HDPAL she is a little nervous about beta blockers because of the frequency of Brady arrhythmias. #NKFClinicals
Summary slide #NKFClinicals

• • •
Missing some Tweet in this thread? You can try to
force a refresh