Emily Oster’s 2005 article, “Treating HIV Doesn’t Pay” rightfully appalls people for the morally bankrupt conclusion of the title. Given the dreadful conclusion, it's something of a relief that Oster's arrival at it is more via deus ex machina than any actual argument. 🧵 

Oster frames her article as if she were answering the question “Is treatment the right solution?” but leaves her reader to wonder “to what problem?” Her initial suggestion is “to maximize life.”

She then moves on to an unfortunate “In other words to save the most years of life”; unfortunate because it is not a rephrasing, but something else entirely.

“To maximize life” suggests the extending of an afflicted person’s life expectancy. OTOH, “to save the most years of life" one could simply add an additional year or so to everyone.
With no clear goal in mind, Oster sets off to do some calculations.

She tells us she hates to sound cruel, but numbers don’t lie: “Treatment is not an effective way to combat the epidemic.” With that, we have a new goal, “to combat the epidemic” which has nothing to do with years lived but with the number of infections.
In its way, this is an impressive accomplishment. In a matter of a mere 4 sentences, we are treated to 3 separate goals.
In fact, Oster is not done introducing various goals. Our fourth goal, “preventing AIDS deaths”, comes towards the end.
It’s clear by "preventing AIDS deaths", Oster doesn’t mean preventing AIDS deaths. She’s just told us she isn’t interested in stopping anyone from dying of AIDS. That would require the antiretrovirals she is against.
I’m not one to throw up my hands so let’s just assume Oster managed to say what she means: her interest is in reducing infections. Treating them is, Oster tells us, “clearly the most expensive option.” It’s the most expensive because it has the highest price tag, $365/life-year.
On the other hand, preventing infections by using antibiotics to heal the sores through which HIV infects, costs only $3.65/per life-year.
The other preventative, education, costs $16/life-year.

Having laid out the costs, it’s conclusion time and the end of antiretrovirals as far as Oster is concerned.
But what sort of cash-register economics is this where the only consideration is a price-tag considered once? Some costs are off-set by benefits. Some costs are ongoing. We aren't at all done.
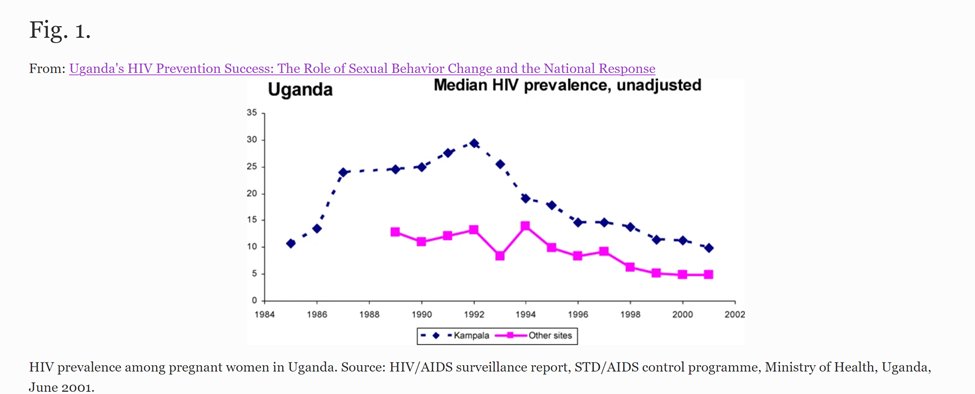
Take education. Oster considers Uganda’s successful education campaign, but only as a way of arriving at the $16/life-year cost.
That doesn’t take into account the considerable bang-for-the-buck Uganda got by educating, not just about AIDS, but condom use and STDs. Those benefits are had for the same $16.00 investment. academic.oup.com/her/article/16…

And let’s not overlook that the offspring of those educated will benefit from lessons learned by their parents. I get that Oster left benefits out, but I just don’t think that’s a good idea.
Now consider antibiotics. They treat one infection at a time. But people get reinfections, requiring antibiotics over and over. What’s the cost of that & wouldn’t someone eventually think education is called for - if only to suggest condoms? So, wouldn't we be educating anyway?
Considering antiretrovirals, Oster is too quick by half dismissing them solely on price. After all, giving every infected person antiretrovirals immediately would end the epidemic in 6 months.
On the other hand, Uganda’s educational campaign, which began in 1986, took years to pay off and all the while costs of, at least comforting the infected, are accumulating.
There’s another problem for Oster. The people Oster tells us aren’t worth treating are going to die. They will die of AIDS, they will die young and they won’t die for free. No one, no hospital, no doctor, lets a young person go without a fight. And that fight is expensive.
On the other hand, a person treated with antivirals might just live long enough to die for free; that is, as we all want to: at home, comfortable and with our loved ones. This offsets the cost of antiretrovirals.
I am not a fan of cost-benefit analysis. I find these gritty details disturbing but I engage with them to make a point: if you are going to do a cost benefit analysis, for heaven’s sake do it right. And if your conclusion is repugnant, be extra right.
But Oster hasn't done a cost-benefit analysis. By way of arguing for a point, she hasn't done much at all. Instead, having no argument, the focus of criticisms of the article have been on Oster herself: her and her repugnant conclusion. She earned this.
The article is here.
forbes.com/forbes/2005/07…
forbes.com/forbes/2005/07…
@threadreaderapp please unroll.
• • •
Missing some Tweet in this thread? You can try to
force a refresh