1/ After 2 years of working hard to avoid getting-- and spreading-- COVID, the pandemic finally caught up with my family.
I thought I would share some of the things I learned along the way.
I thought I would share some of the things I learned along the way.

2/ *Infection*
Our behavior didn't change, but the virus did. As @ScottGottliebMD has noted- it sure seems like the most recent BA2 surge is increasingly hitting the remaining uninfected, who've been limiting social interactions, social distancing, masking
Our behavior didn't change, but the virus did. As @ScottGottliebMD has noted- it sure seems like the most recent BA2 surge is increasingly hitting the remaining uninfected, who've been limiting social interactions, social distancing, masking
https://twitter.com/Farzad_MD/status/1471631913714688008?s=20&t=cRKCpnjsU7ZcI5gnnR_mnQ
3/ My elderly parents have been essentially home-bound for the past 2 years, with very limited number of contacts.
We still don't know exactly how my dad got it. 🤷♀️
But I am so grateful that we delayed his infection until he had a chance to get vaccinated and boosted 🙏
We still don't know exactly how my dad got it. 🤷♀️
But I am so grateful that we delayed his infection until he had a chance to get vaccinated and boosted 🙏
4/ *Symptoms*
We had what you would expect- initial chills, bodyaches, then runny nose
My dad had a cough very early, I had it later, but quite persistent (I still have it 3 weeks later)
A symptom I didn't expect was wheezing. I didn't measure peak flows but would have been bad
We had what you would expect- initial chills, bodyaches, then runny nose
My dad had a cough very early, I had it later, but quite persistent (I still have it 3 weeks later)
A symptom I didn't expect was wheezing. I didn't measure peak flows but would have been bad
5/ I was basically fine after day 2. (53 yo)
My dad (86 yo) didn't need to be hospitalized but he got pretty sick for a while.
Without good care at home, and certainly without the vaccine and booster and therapeutics (more on this) I could easily have imagined a bad outcome.
My dad (86 yo) didn't need to be hospitalized but he got pretty sick for a while.
Without good care at home, and certainly without the vaccine and booster and therapeutics (more on this) I could easily have imagined a bad outcome.
6/ *Diagnosis*
PCR is more sensitive early on in the course- but delays in reporting make it useless compared to rapid antigen.
I got a pharmacy drive-thru PCR test (by @verilylifesci), but it took 3 days for the results to come back positive
Rapid antigen test + next day
PCR is more sensitive early on in the course- but delays in reporting make it useless compared to rapid antigen.
I got a pharmacy drive-thru PCR test (by @verilylifesci), but it took 3 days for the results to come back positive
Rapid antigen test + next day
7/ I was trying to get confirmatory PCR test for my dad, but only same-day service was a for-profiteering place that charged $250
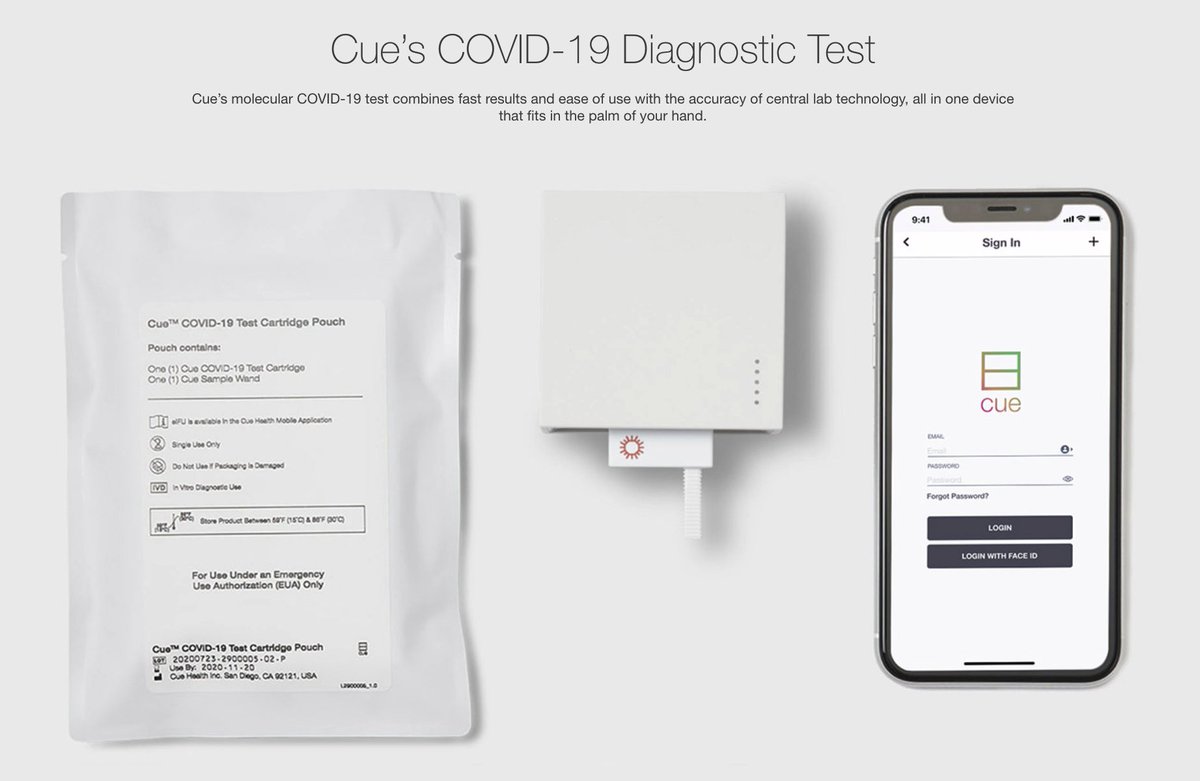
I actually ended up buying a @CueHealth 15 minute home PCR machine ($70 a cartridge)- which is an amazing device, but ended up not mattering
I actually ended up buying a @CueHealth 15 minute home PCR machine ($70 a cartridge)- which is an amazing device, but ended up not mattering
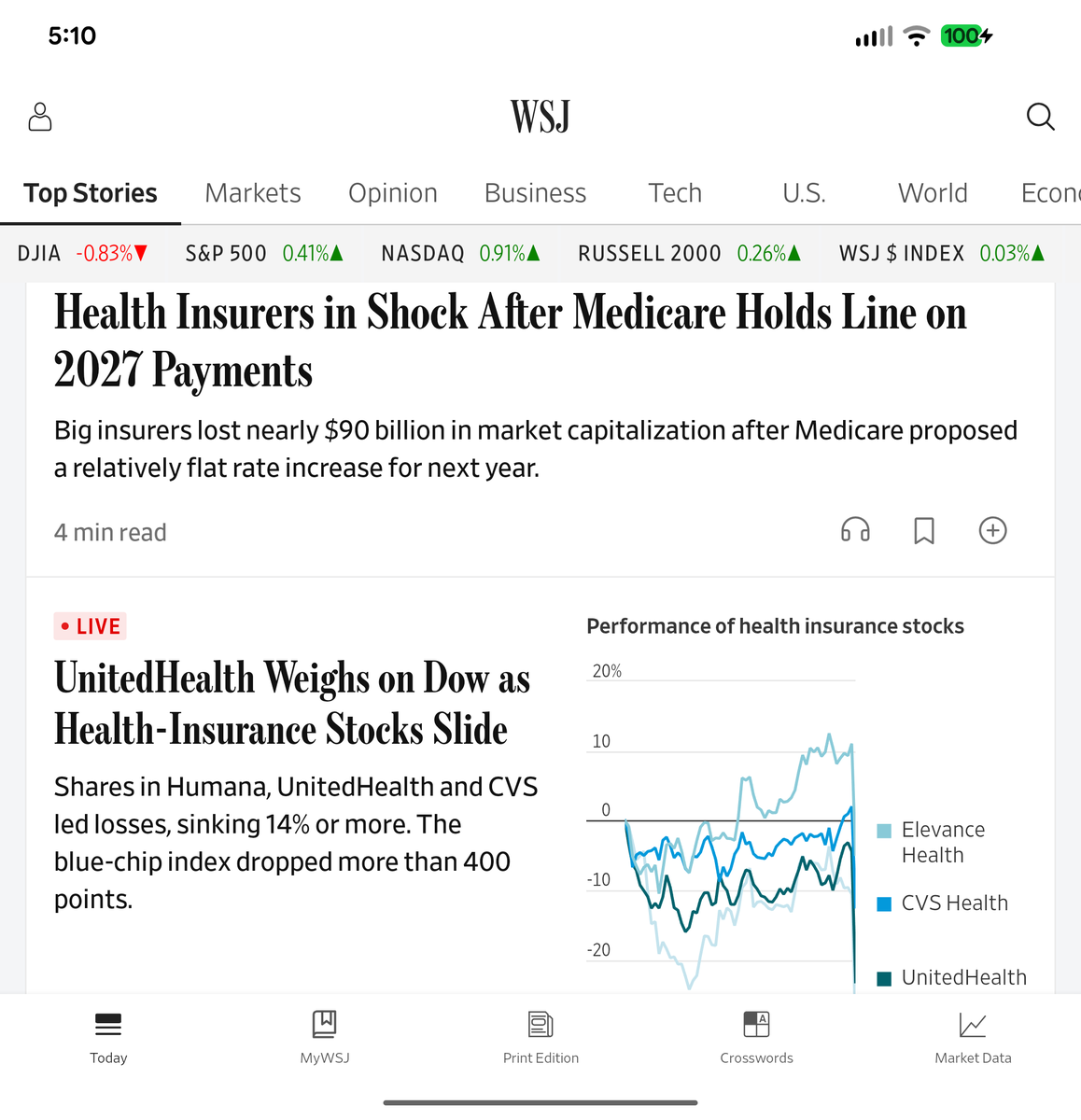
8/ *Therapeutics
I am SO GLAD for science, and that we delayed his infection until Paxlovid was widely available.
Pharmacies all had it in stock
But getting a prescription from his academic medical center PCP quickly was beyond my abilities
Portal messages, answering system 👿
I am SO GLAD for science, and that we delayed his infection until Paxlovid was widely available.
Pharmacies all had it in stock
But getting a prescription from his academic medical center PCP quickly was beyond my abilities
Portal messages, answering system 👿
9/ Here's the hack- schedule a virtual urgent care visit
it's faster than getting a message to the PCP who knows him best. The urgent care nurse ran through checklist, and quickly agreed he qualified
One problem- they want a recent (last 6 mos) renal function test for dosing
it's faster than getting a message to the PCP who knows him best. The urgent care nurse ran through checklist, and quickly agreed he qualified
One problem- they want a recent (last 6 mos) renal function test for dosing
10/ I ended up convincing them that his most recent test (9 mons ago) already showed moderate renal impairment, so let's just go with the renal dosing already, and get the pills started today.
The instructions are a bit hard to follow- so they put a sticker on the blister pack
The instructions are a bit hard to follow- so they put a sticker on the blister pack
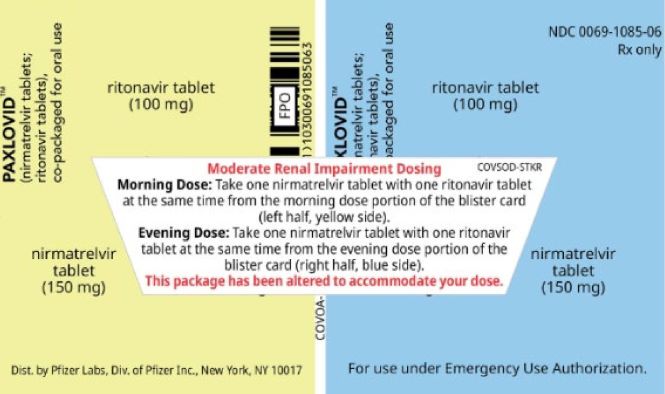
11/ make sure you take it correctly!
You have to "take one of each color" pill, but the color on the back can confuse things-
I heard of one person whose family gave them 2 ritonavir tabs in the morning, and 2 nirmatrevlir tabs at night
That ... won't work
You have to "take one of each color" pill, but the color on the back can confuse things-
I heard of one person whose family gave them 2 ritonavir tabs in the morning, and 2 nirmatrevlir tabs at night
That ... won't work
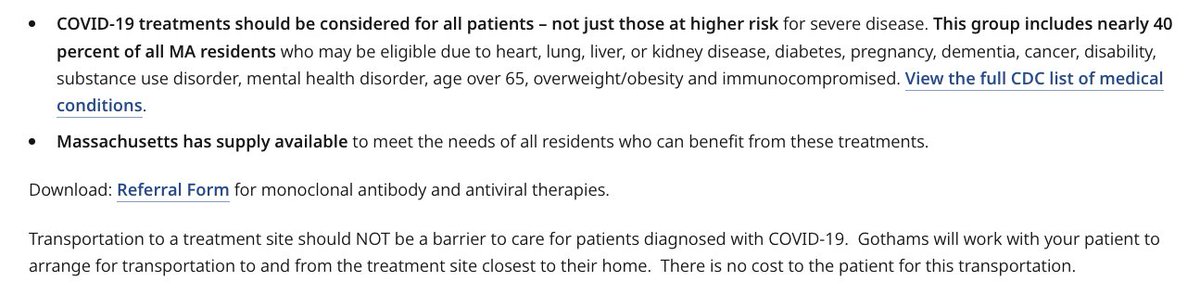
12/ Treatment option #2- Monoclonal Antibodies
My mom got COVID next.
My goal was to get her monoclonals quickly-
"Bebtelovimab should be used as the monoclonal antibody of choice in regions where BA.2 is the dominant subvariant if preferred therapies are not feasible"
My mom got COVID next.
My goal was to get her monoclonals quickly-
"Bebtelovimab should be used as the monoclonal antibody of choice in regions where BA.2 is the dominant subvariant if preferred therapies are not feasible"
13/ Once again, even though there isn't *that much* supply, there's no shortage!
Why?
You have to know how to navigate the system to get it.
Again, forget about calling your PCP office to arrange for it, even if they are within one of the blessed academic institutions
Why?
You have to know how to navigate the system to get it.
Again, forget about calling your PCP office to arrange for it, even if they are within one of the blessed academic institutions

14/ The concept of "urgent primary care" is a non-starter in normie medicine, it seems
The patient portal forces you to choose "non-urgent medical question"
the call line takes a message, but tells you it could take 24-48 hrs to get a response.
"Go to the Emergency Room" sucks
The patient portal forces you to choose "non-urgent medical question"
the call line takes a message, but tells you it could take 24-48 hrs to get a response.
"Go to the Emergency Room" sucks
15/ NB- I'm CEO of @AledadeACO and our 1,000+ independent primary care practices coach their patients "Call us 1st!" - it's easy to see how that would translate into 14% fewer ED visits, 15% lower hospitalizations, and a lot less suffering.
But that's not most of the world
But that's not most of the world
16/ so... I called the MA Dept Public Health at the minute they opened on 8 am Monday morning, and got a reservation for a Monoclonal Ab infusion that day at 2 pm.
Not charge. They can help with wheelchairs/ transportation.
But you have to know how to work the system
Not charge. They can help with wheelchairs/ transportation.
But you have to know how to work the system
17/ My mom's response to the mAb was impressively fast.
I went from pretty worried about her clinically to completely at ease within 24 hours.
I think they are massively underused right now.
If you have an elderly/ at risk loved one with COVID infection, I'd try to get it.
I went from pretty worried about her clinically to completely at ease within 24 hours.
I think they are massively underused right now.
If you have an elderly/ at risk loved one with COVID infection, I'd try to get it.
18/ *Leaving Isolation
The CDC advice to leave isolation after 5 days without requiring negative rapid antigen test is ... unsupported by the science IMO
My dad was still antigen+ (infectious) until Day 8. Should he have returned home to sleep next to my 83yo mom on Day 5?
No
The CDC advice to leave isolation after 5 days without requiring negative rapid antigen test is ... unsupported by the science IMO
My dad was still antigen+ (infectious) until Day 8. Should he have returned home to sleep next to my 83yo mom on Day 5?
No
19/ I still feel bad that I wasn't even more careful to leave a longer buffer
My mom tested positive a week after my dad came home when he turned antigen negative
We can't be sure where she got it from, but it sure seems likely that it was residual shedding from my dad.
My mom tested positive a week after my dad came home when he turned antigen negative
We can't be sure where she got it from, but it sure seems likely that it was residual shedding from my dad.
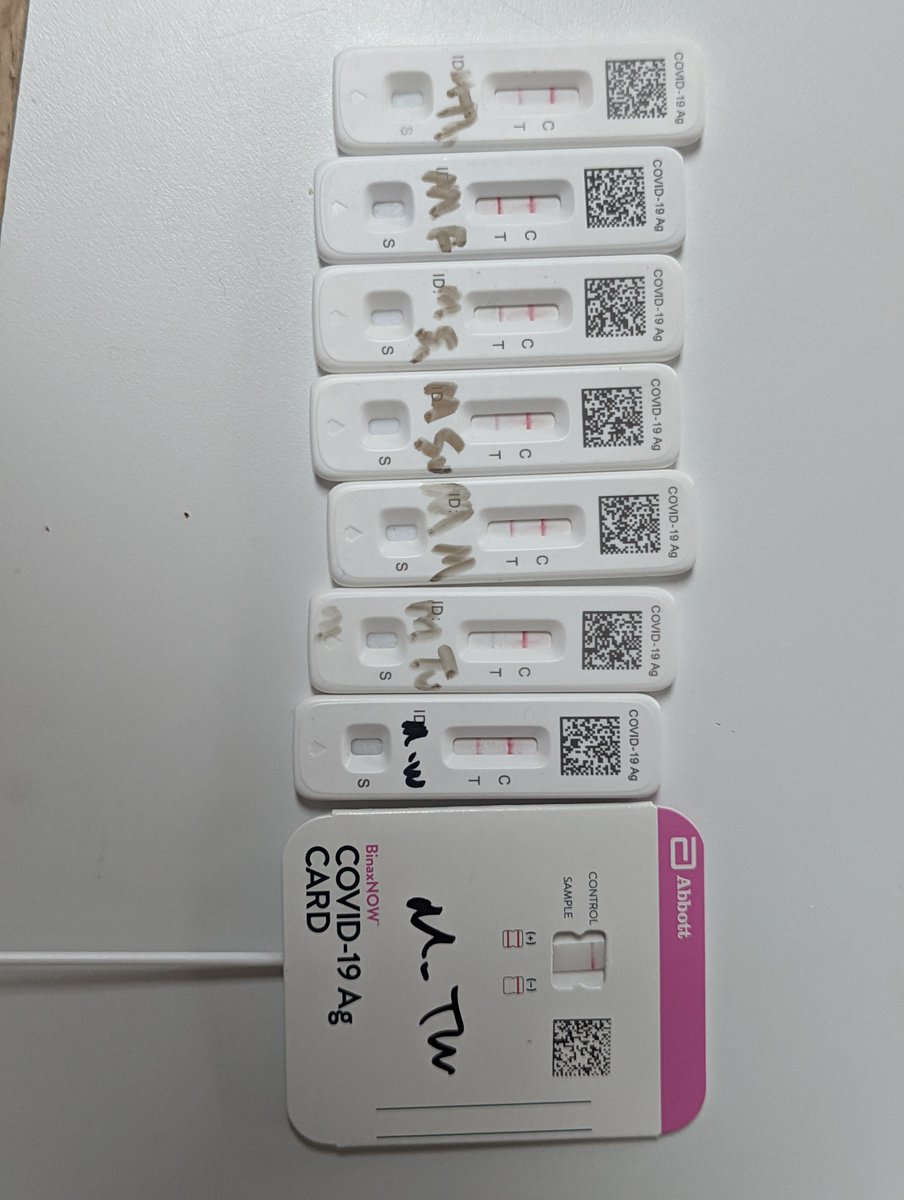
20/ I was still antigen positive on day 5
I was still antigen + on Day 10, so I drove home 10 hours instead of flying on commercial (OK per CDC)
I isolated & masked & ventilated around my household members until I turned negative... on Day 15!
Thankful I didn't give it to them
I was still antigen + on Day 10, so I drove home 10 hours instead of flying on commercial (OK per CDC)
I isolated & masked & ventilated around my household members until I turned negative... on Day 15!
Thankful I didn't give it to them

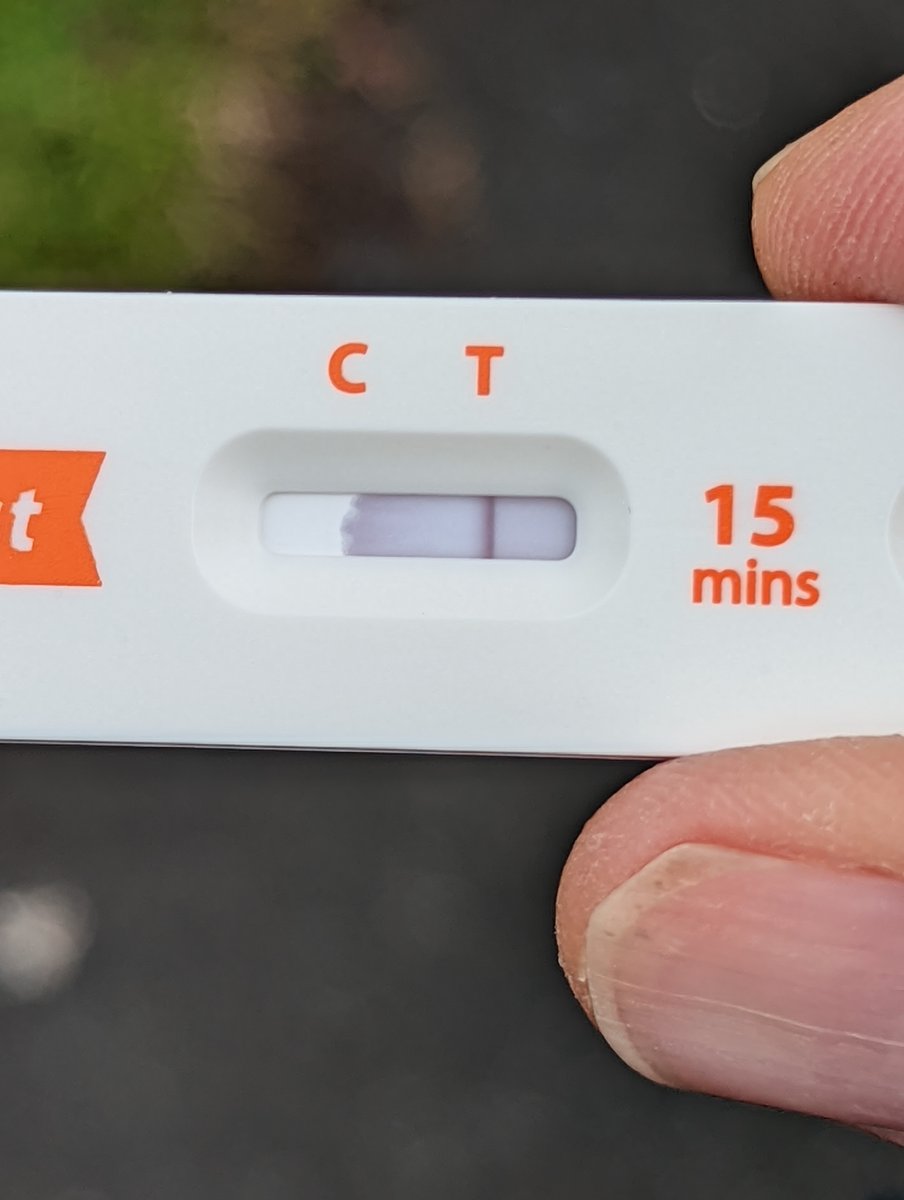
21/ It's impressive when you see a really strong positive antigen test
The Test stripe turns positive almost instantly as the fluid hits it
You can see here (on Day 12) how positive the test is within seconds-so quickly that the fluid hasn't even had a chance to hit the Control
The Test stripe turns positive almost instantly as the fluid hits it
You can see here (on Day 12) how positive the test is within seconds-so quickly that the fluid hasn't even had a chance to hit the Control
22/ It's nuts how misunderstood this is, even by medical professionals and institutions who should know better.
PCR tests will stay positive long after you are no longer infectious.
THAT'S NOT TRUE FOR RAPID ANTIGEN TESTS.
If you're antigen positive, assume you're infectious
PCR tests will stay positive long after you are no longer infectious.
THAT'S NOT TRUE FOR RAPID ANTIGEN TESTS.
If you're antigen positive, assume you're infectious
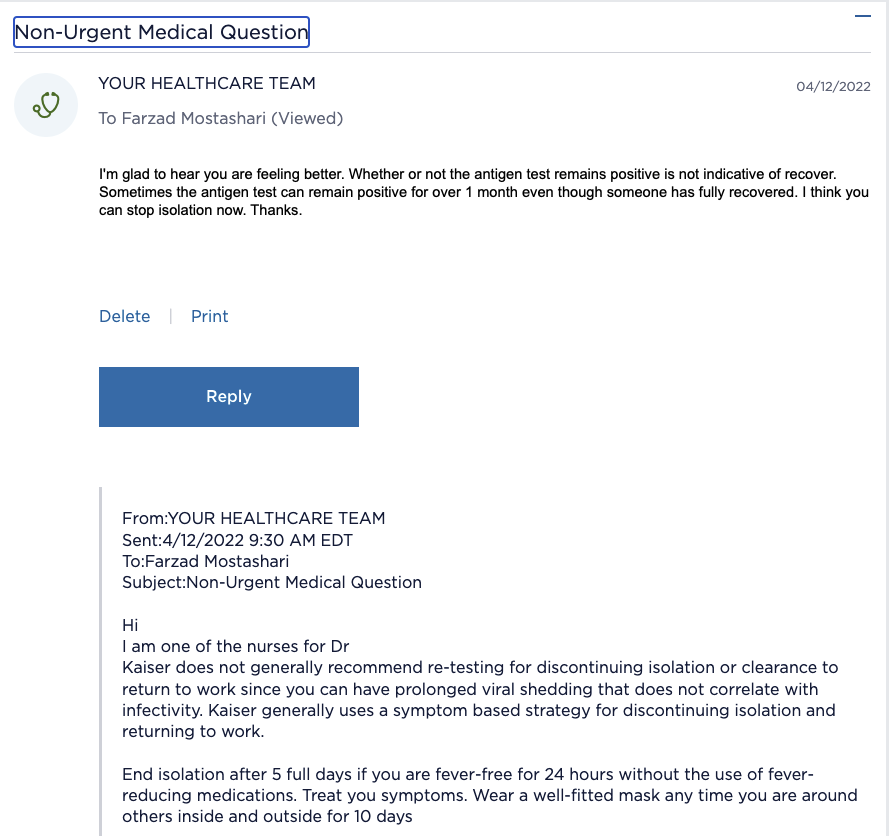
23/ Here is wrong advice from @KPMemberService
I generally think Kaiser-Permanente has excellent evidence-based, data-driven care (which is why I'm a member)
But I've been frankly disappointed with their COVID response in proactive vaccine distribution, therapeutics, or this👇
I generally think Kaiser-Permanente has excellent evidence-based, data-driven care (which is why I'm a member)
But I've been frankly disappointed with their COVID response in proactive vaccine distribution, therapeutics, or this👇
24/ We are all fine, thanks to vaccines (and my ability to work the system to get my parents therapeutics right away)
But it shouldn't be this hard.
Renal tests before Paxlovid is a problem.
Inability to reach PCPs urgently is terrible,
Leaving isolation without - Ag is nuts
But it shouldn't be this hard.
Renal tests before Paxlovid is a problem.
Inability to reach PCPs urgently is terrible,
Leaving isolation without - Ag is nuts
25/ Special thanks to all my friends and experts who helped guide me and comfort us during this time, but especially @bijans and @FranklinHuang
26/ I forgot to add- *Side Effects
Monoclonal had zero side effects
Paxlovid has very unpleasant bitter/metallic taste and stomach cramps/ diarrhea
(be careful of elderly people risk of falls if rushing to bathroom while weakened, consider walker use)
Monoclonal had zero side effects
Paxlovid has very unpleasant bitter/metallic taste and stomach cramps/ diarrhea
(be careful of elderly people risk of falls if rushing to bathroom while weakened, consider walker use)
27/ *Costs
My parents have Medicare and supplemental insurance, and we could certainly afford tests or treatments, but very grateful that the medications and antibody infusion are free- paid for by the government to remove financial barriers
+They got 8 free rapid antigen tests
My parents have Medicare and supplemental insurance, and we could certainly afford tests or treatments, but very grateful that the medications and antibody infusion are free- paid for by the government to remove financial barriers
+They got 8 free rapid antigen tests
28/ *note/context
They love their PCP, who is smart, hard working, and cares a lot for them
It's just that her organization has made a conscious decision to make it hard for patients to reach her and communicate with her directly
It's more "efficient" fee-for-service that way
They love their PCP, who is smart, hard working, and cares a lot for them
It's just that her organization has made a conscious decision to make it hard for patients to reach her and communicate with her directly
It's more "efficient" fee-for-service that way
29/ *Care @home
1) managing meds. Including decisions re taking/not taking regular meds (eg drug interaction between Paxlovid & statins)
2) monitoring vitals, symptom trends (like difficulty breathing) to decide if need to go to ER
3) ensuring food/water intake
4) falls prev
1) managing meds. Including decisions re taking/not taking regular meds (eg drug interaction between Paxlovid & statins)
2) monitoring vitals, symptom trends (like difficulty breathing) to decide if need to go to ER
3) ensuring food/water intake
4) falls prev
30/ the excellent @bijans has made a terrific guide that summarizes key steps to navigating therapeutics for your at-risk loved ones with covid
https://twitter.com/bijans/status/1515335811994206221?t=7sqyanEf48Wi5n0KkKM5Pg&s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh