Next up in the #Tweetorial series based on my Hemodynamic Rounds Live lectures I’ll be discussing the basics of mechanical circulatory support (MCS) 📚
There is a lot of info to cover so this #Tweetorial will be broken up into four parts.
Follow along below for part 1. ⬇
There is a lot of info to cover so this #Tweetorial will be broken up into four parts.
Follow along below for part 1. ⬇

In this #Tweetorial I will go through the basics of LV function metrics – how do we measure them; how do we understand them & how do we apply them? 📊
Then we will examine what each device is supposed to do for LV function & understand a couple of pathologic conditions.
Then we will examine what each device is supposed to do for LV function & understand a couple of pathologic conditions.
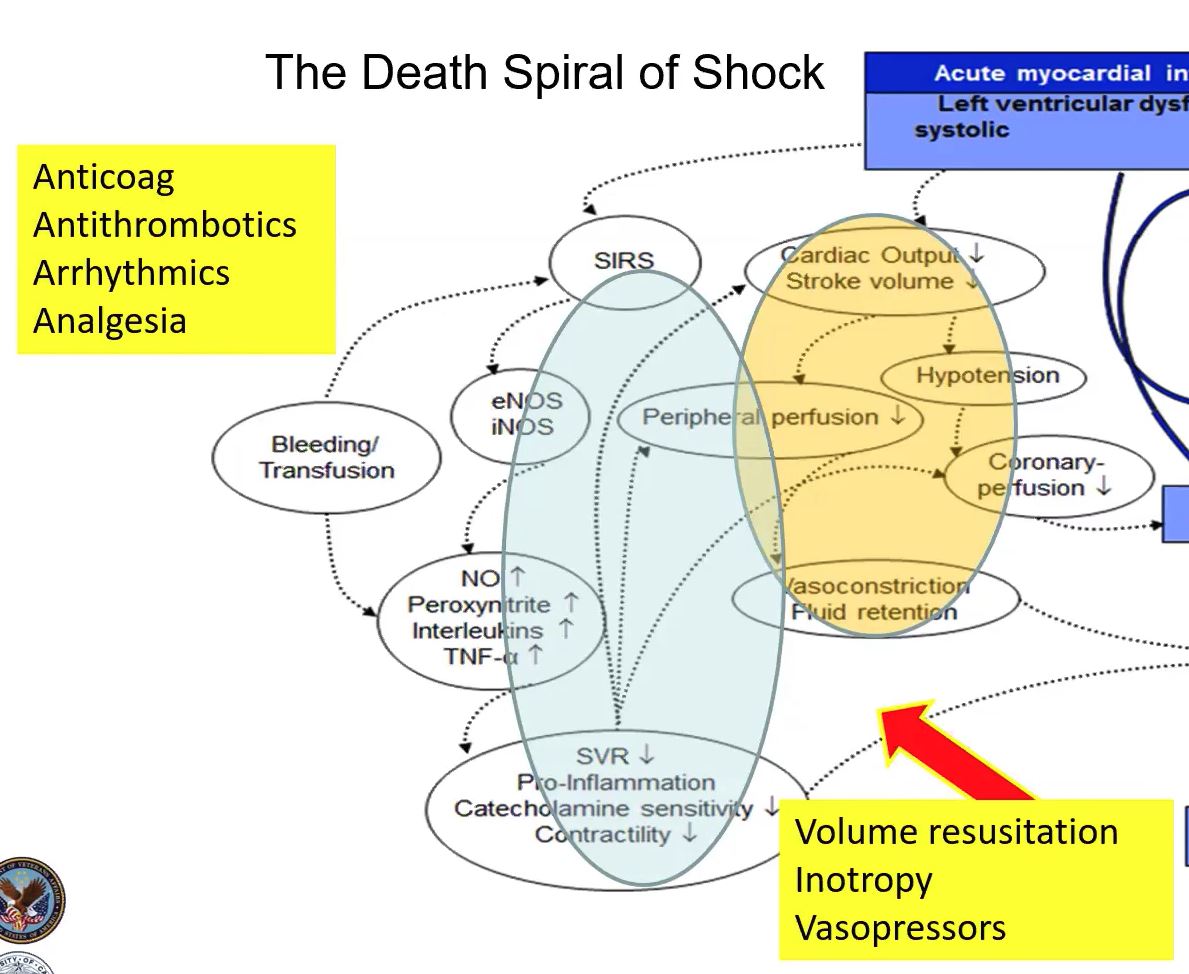
We’ll start by reviewing shock, its spiral down to death, & the factors involved. ➰ We’ll also see where hemodynamic support really plays a role.

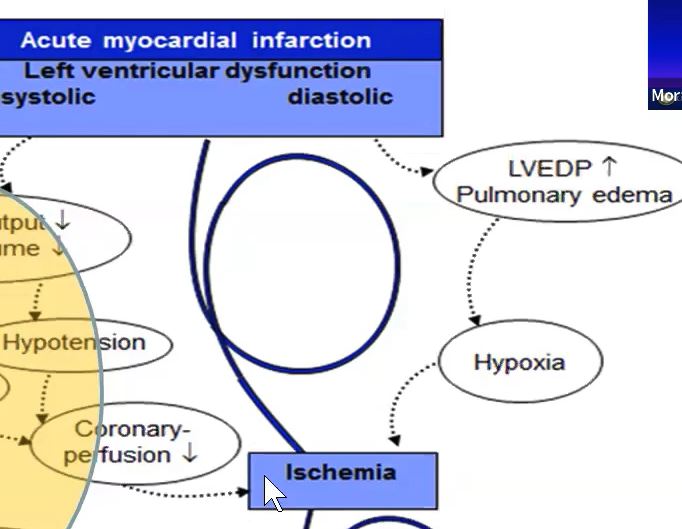
In AMICS, the first event that occurs is myocardial infarction – severe impairment of left ventricular function. 💔
Two things happen - Systolic impairment & diastolic impairment. 🛑
Two things happen - Systolic impairment & diastolic impairment. 🛑
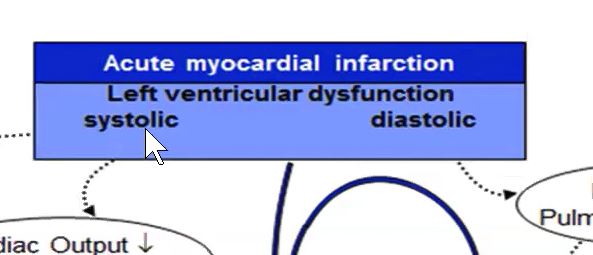
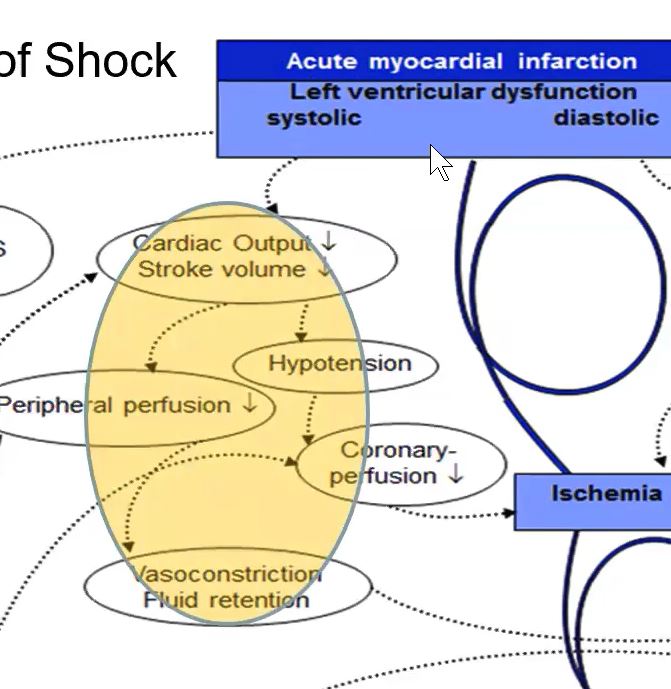
With systolic impairment, cardiac output & stroke volume fall. 📉
Hypotension results. Peripheral & coronary blood flow becomes impaired.
The response to this is systematic vasoconstriction & fluid retention. 💧
Hypotension results. Peripheral & coronary blood flow becomes impaired.
The response to this is systematic vasoconstriction & fluid retention. 💧
A dramatic fall in the systematic perfusion 💨 & the release of biomarkers & systemic inflammatory response comes next. Biomarkers such as eNOS, iNOS, TNF-a, pro-inflammatory materials reduces further contractility. ⬇
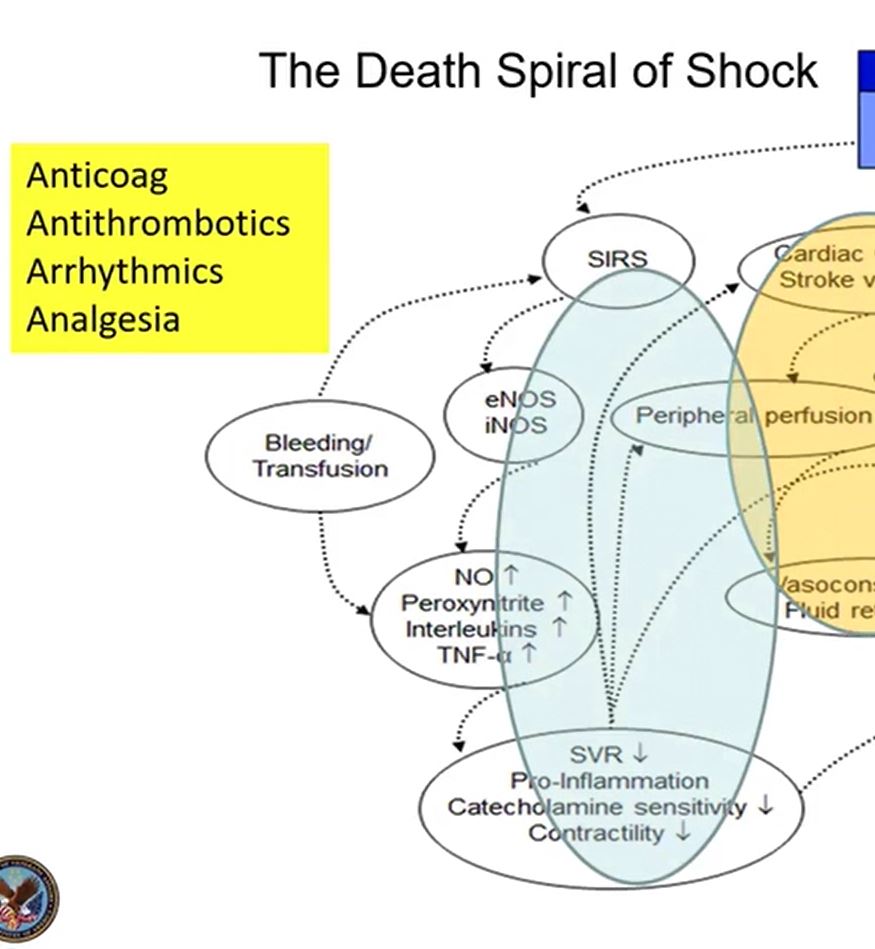
We address these two areas with all medical therapies ⚕ – Anticoagulants, Arrhythmics, etc. and provide volume resuscitation, inotropy & vasopressors, but that doesn’t always work. 💊
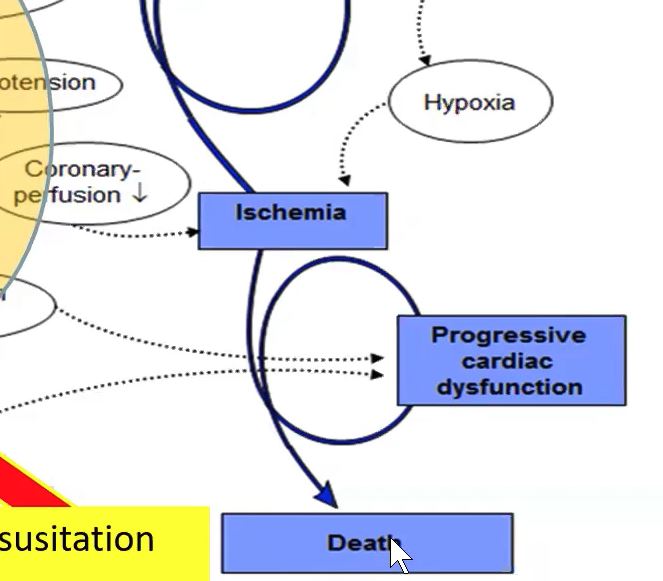
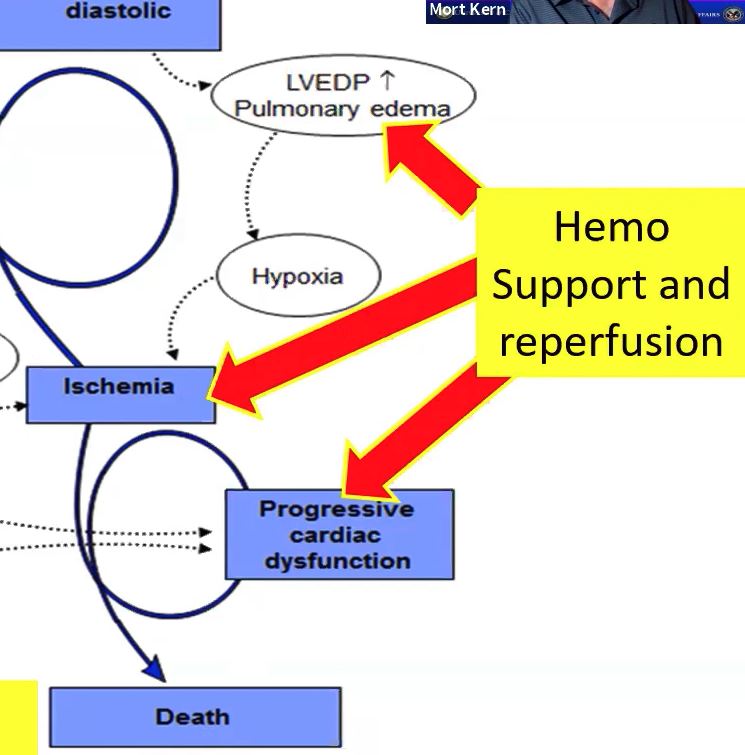
On the LV diastolic side of the shock cascade - LVEDP goes up as a compensatory mechanism.📈 This causes LA & PV pressure to ⬆ which can cause pulmonary congestion. Hypoxia results, which further promotes ischemia in combination with decreased perfusion. This must be stopped.🚫
If this cascade isn’t stopped progressive cardiac dysfunction & death occurs.
At this point we hemodynamic support can be introduced in addition to coronary reperfusion. ⛽
The hemodynamic syndrome of shock ⚡ evolves into a HemoMetabolic syndrome (a term coined by @NavinKapur4). If left unabated shock produces end organ damage and multisystem failure. 🤕
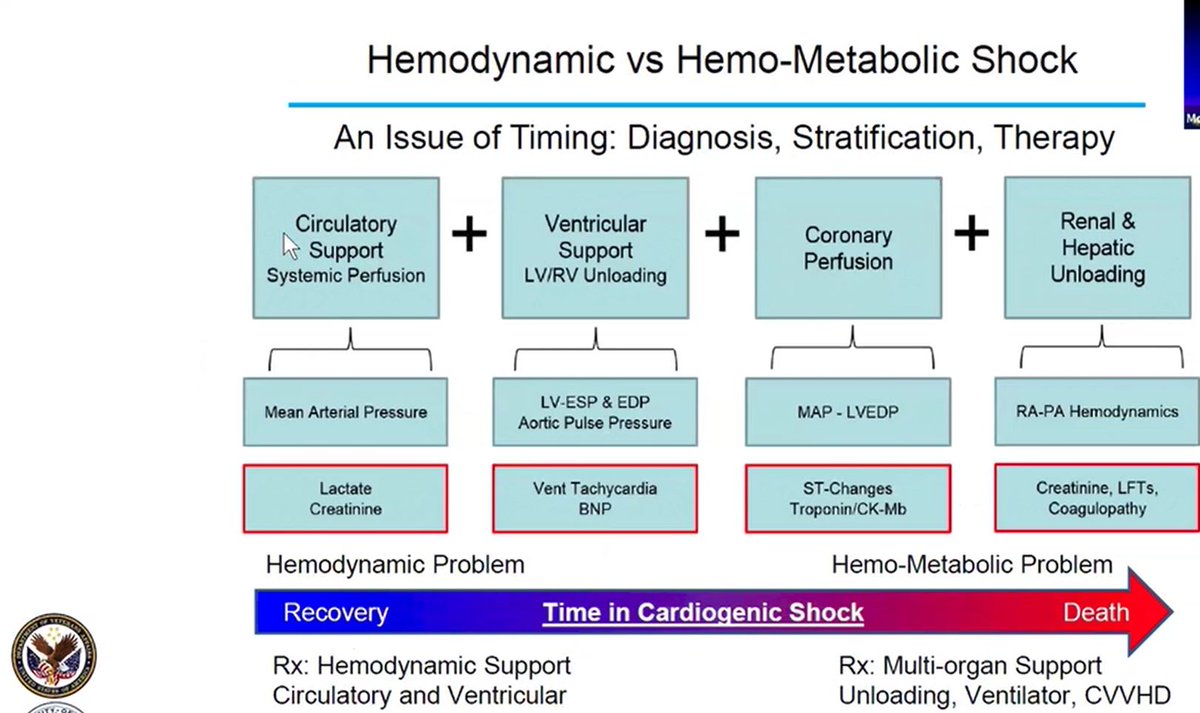
With circulatory support & systemic perfusion as an early goal to achieve recovery, we focus on normalizing mean arterial pressure. We measure lactates & creatinine to assess the HemoMetabolic state and to evaluate the patient’s prognosis. 📊
AMI shock necessitates ventricular support & sometimes both LV & RV support & unloading. We measure these looking at filling pressures – The LV with the wedge or PCWP and the RV with RA pressure measurements.
Because of decreased MAP and ⬆ LVEDP there is impairment in coronary perfusion resulting in EKG changes & Troponin 📈.
Finally, as impairment of perfusion persists, renal & hepatic unloading is needed - if we can do it. We see elevation of right sided pressures, abnormal PA hemodynamics, abnormal coagulopathy & liver functions. 🌋
The likelihood of heart recovery is much better the earlier we evaluate and intervene on patients with shock. 👈⌛
If the hemodynamic & metabolic events don’t change the patient will die. That again supports the use of MCS. ⚙⛽
If the hemodynamic & metabolic events don’t change the patient will die. That again supports the use of MCS. ⚙⛽

This concludes part 1 of this #Tweetorial on the Basics of MCS.
Stay tuned for part 2, when we will examine different device options.
Stay tuned for part 2, when we will examine different device options.
• • •
Missing some Tweet in this thread? You can try to
force a refresh