1) A 🧵 providing a whistle stop tour of Frozen Shoulder (FS) 

2) FS is associated with stiffness of the capsule which restricts GHJ A/PROM within a capsular pattern coupled with a normal XR finding (Zuckerman 2011). Previously thought to be self-limiting, now ++ evidence highlighting the significance it has on pain, disability and function

3) Epidemiology: Thought to affect 2-5% of the gen pop between the age of 40-70yrs. Women are more susceptible & it is thought that 6-17% of patients are unfortunate enough to develop it in the contralateral arm within the first 5yrs (Dyer et al., 2021).
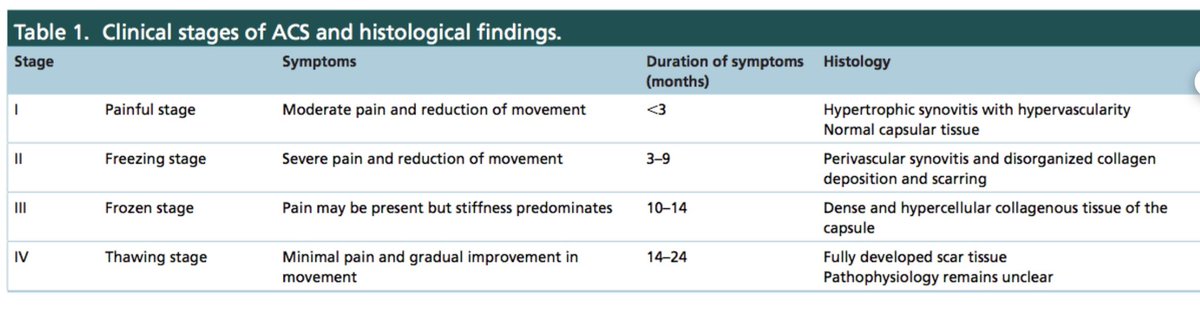
4) Exact pathophysiology is not fully understood, yet histological findings highlight a thickened & tight capsule w chronic inflammatory cells & fibroblasts found in the joint capsule which suggest an autoimmune component (Date & Rahman 2020). This table shows the 4 stages;
5) It is split into two types, a) primary - idiopathic onset of Sx & b) secondary - ? associated with metabolic syndrome as a large % are obese, there is a x5 more chance of FS if diabetic. Thyroid problems, previous surgery, dupuytrens etc are also related (Date + Rahman 2020).
6) Diabetes & FS; T1DM = causal risk factor for developing FS (Green et al., 2021). 13.4% prevalence of FS in diabetics & 30% of FS population are diabetic (Dyer et al., 2021). ? glycemic changes influence capsular stiffness through collagen & release proinflammatory cytokines
7) Features; Pain is often severe, disabling and impedes sleep during the initial stage. Locality can vary, described as deep & may refer to the bicep/elbow. As the capsule stiffens, ROM is affected & this causes significant functional limitations. This paper summarises it nicely

8) Dx; ‘Shoulder pain for 1/12, unable to lie on affected side with restricted A/PROM, with a minimum of 50% reduction in passive external rotation vs contralateral side (Kelley et al., 2013). *Often assessing in supine, w a towel under the elbow helps prevent any compensation*

9) Imaging: Often not needed for a Dx. XR is recommended to rule out OA, # / dislocation or more sinister pathology. US may detect thickening of the rotator interval / surrounding soft tissue or teno/synovitis.
10) Prognosis; Will vary from pt-pt. Previous thoughts were that it has a favourable natural Hx. Yet Schaffer et al (1992) found 50% had Sx still at 7yrs. Whereas Wong et al (2017) showed ER remained limited by approx 50% at 1yr f/u if left untreated.
11) Treatment; UK Frost Trial. They concluded injection & PT worked well in unison and this had similar favourable outcomes at 1yr f/u compared to MUA & capsular release. Surgery had the best outcome @ 12/12 but not clinically superior & is associated with risks.

12) For further reading; pubmed.ncbi.nlm.nih.gov/33312703/
• • •
Missing some Tweet in this thread? You can try to
force a refresh