1/ *Case presentation of MSSA osteomyelitis*
...
Expert 1: Clearly we should treat w/ IV ceftriaxone
Expert 2: WHAT?! I would never use ceftriaxone to treat this
...
💭Trainee in the audience: What the heck should I be doing?
This week: teaching management reasoning effectively
...
Expert 1: Clearly we should treat w/ IV ceftriaxone
Expert 2: WHAT?! I would never use ceftriaxone to treat this
...
💭Trainee in the audience: What the heck should I be doing?
This week: teaching management reasoning effectively
2/ This week we will discuss how to teach management reasoning, also sometimes referred to as "therapeutic reasoning."
3/ Management reasoning is more complex than diagnostic reasoning because:
1⃣there's usually more than one "right" answer
2⃣many factors must be considered
3⃣a degree of uncertainty about the diagnosis or "best" choice almost always exists
1⃣there's usually more than one "right" answer
2⃣many factors must be considered
3⃣a degree of uncertainty about the diagnosis or "best" choice almost always exists

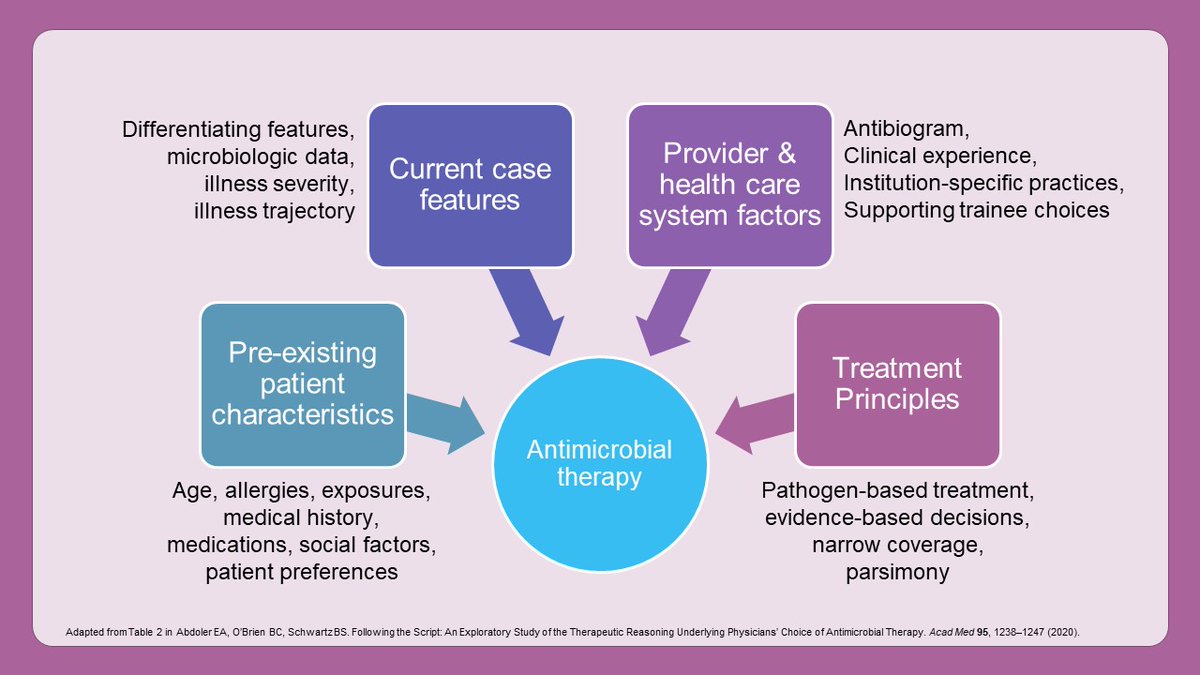
4/ For example, this @AcadMedJournal paper shows that hospitalists and ID physicians consider many different factors when selecting antimicrobials
pubmed.ncbi.nlm.nih.gov/32379146/
pubmed.ncbi.nlm.nih.gov/32379146/
5/ But that's a lot of information to teach all at once, so how can we make teaching this topic more approachable?
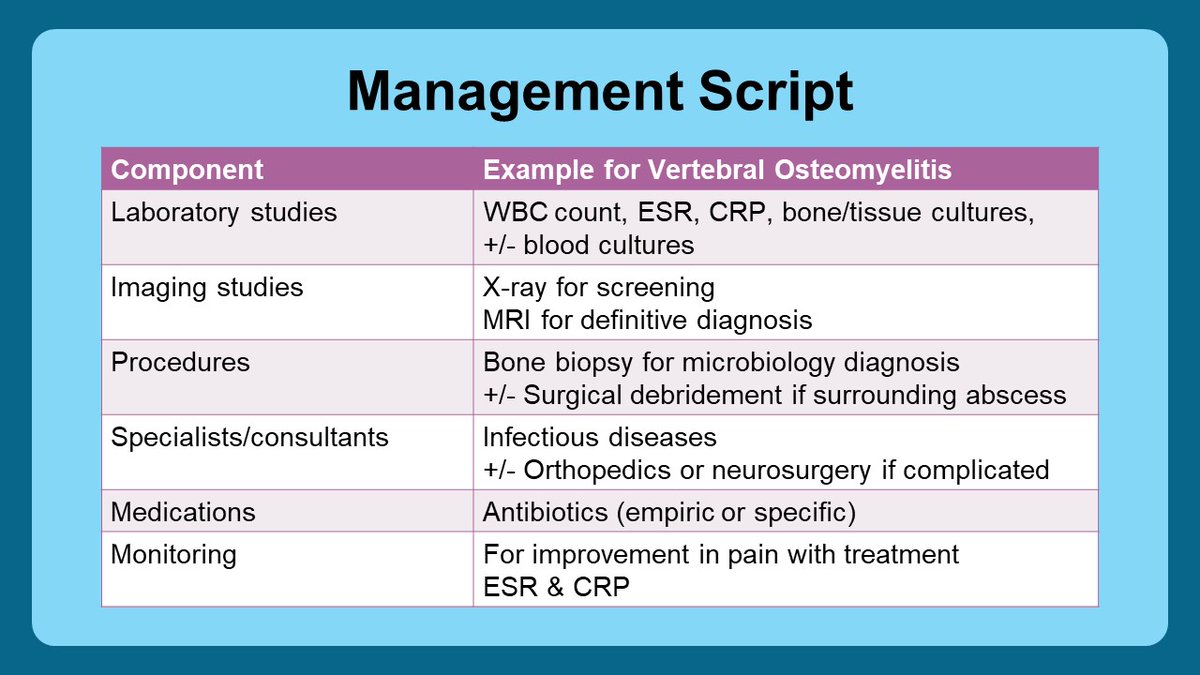
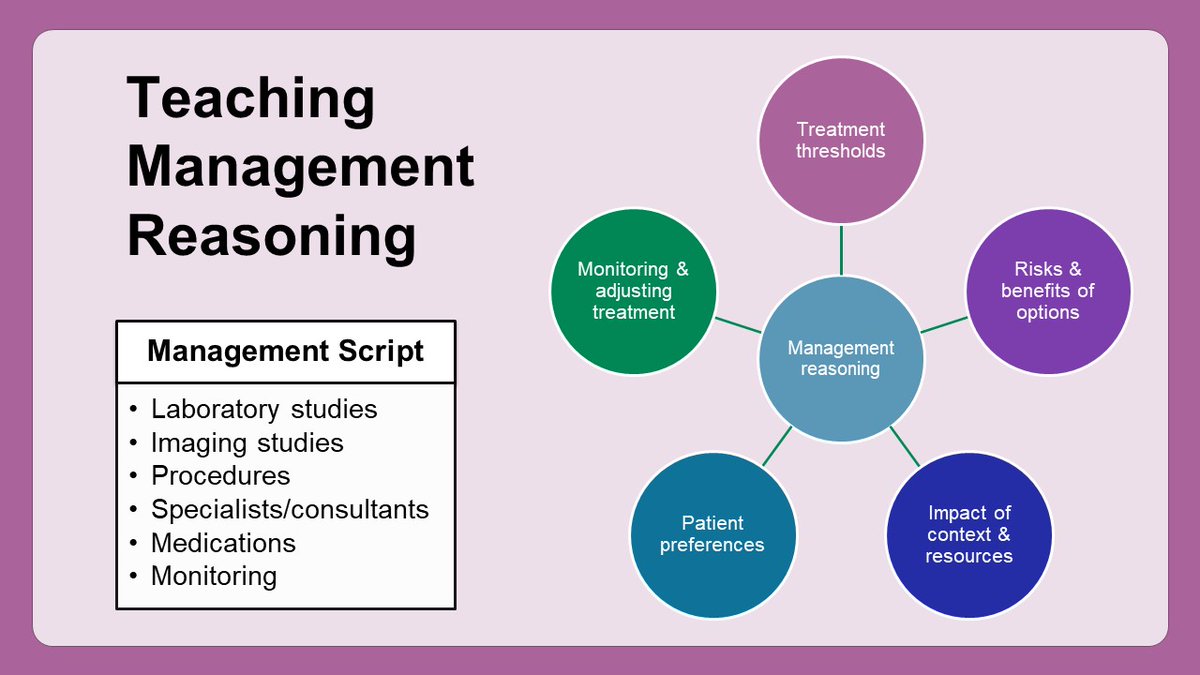
6/ One thing we can teach is a "management script" for common medical conditions, as described by @andrewparsonsMD @thilanMD & @JRencic in this @AcadMedJournal paper:
pubmed.ncbi.nlm.nih.gov/32349018/
Here are the components & an example of what that may look like for osteomyelitis.
pubmed.ncbi.nlm.nih.gov/32349018/
Here are the components & an example of what that may look like for osteomyelitis.
7/ But once our learner’s master the management script, there's so much more we can teach.
And to me, this is the fun part about management reasoning.
And to me, this is the fun part about management reasoning.
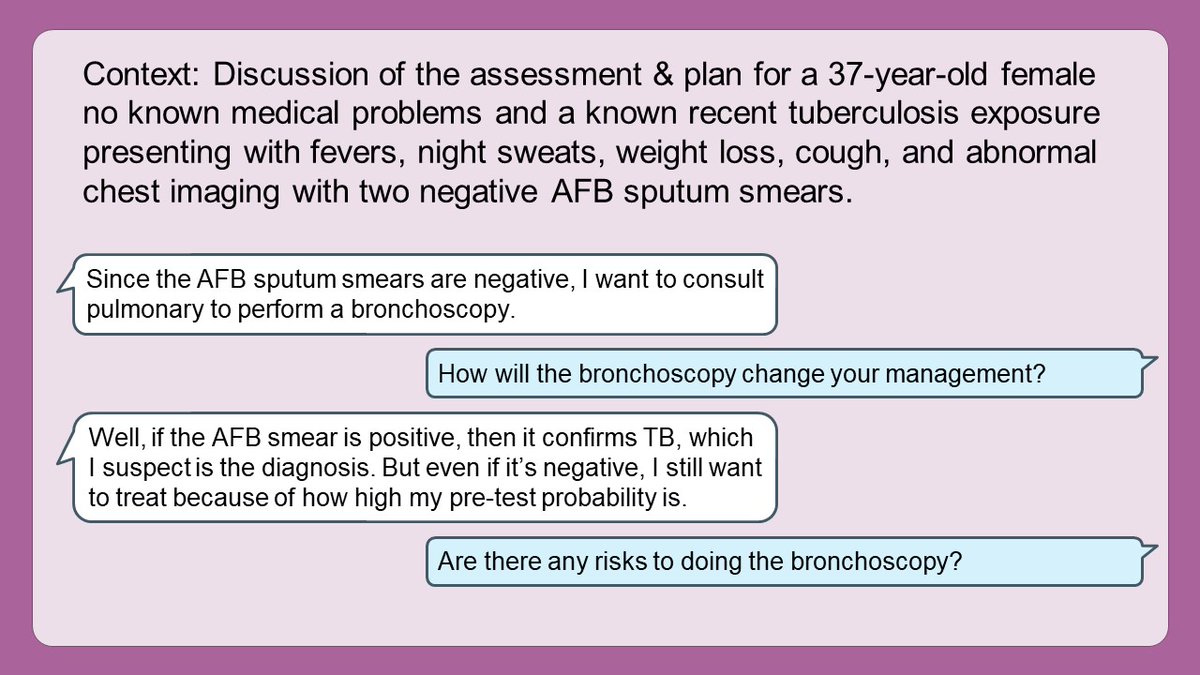
8/ We can teach about testing and treatment thresholds.
For example:
*⃣When do we have enough data to initiate treatment?
*⃣What are the relative risks/benefits of additional testing prior to initiative treatment?
*⃣Will that test CHANGE our management or not?
For example:
*⃣When do we have enough data to initiate treatment?
*⃣What are the relative risks/benefits of additional testing prior to initiative treatment?
*⃣Will that test CHANGE our management or not?
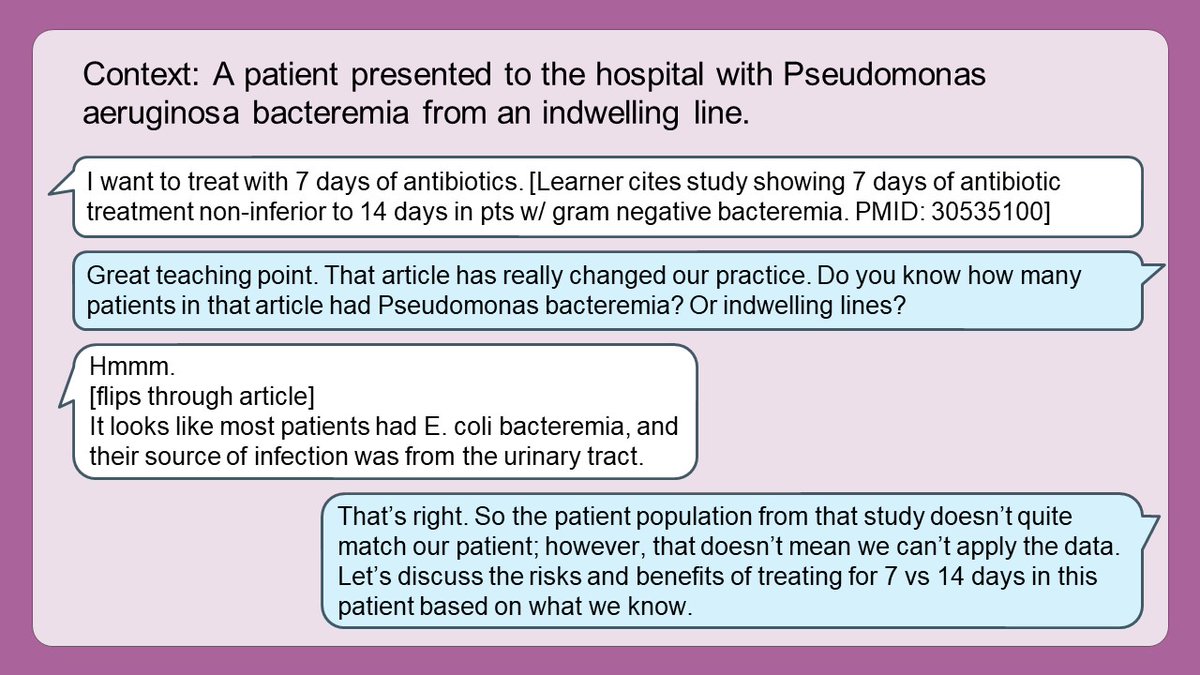
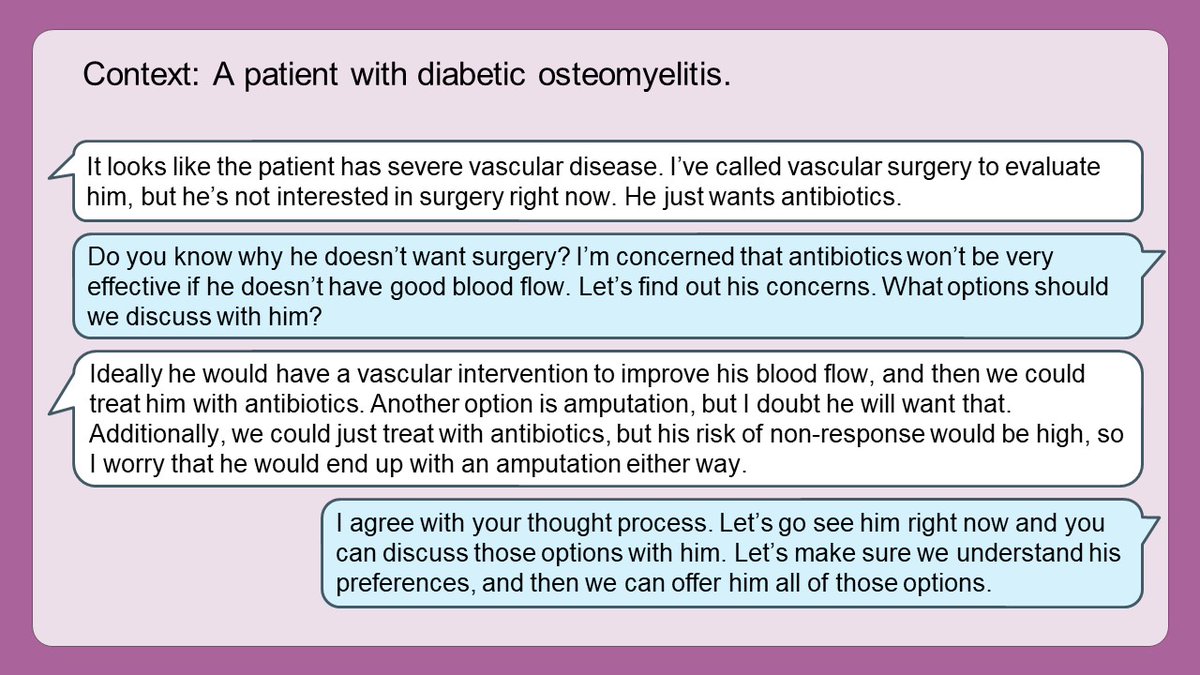
9/ We can also teach about the variety of treatment options.
*⃣What options exist?
*⃣What are the risks/benefits of each?
*⃣How do patient characteristics impact selection? (e.g., medication interactions, allergies, etc.)
*⃣What are the limitations in the data that we have?
*⃣What options exist?
*⃣What are the risks/benefits of each?
*⃣How do patient characteristics impact selection? (e.g., medication interactions, allergies, etc.)
*⃣What are the limitations in the data that we have?
10/ We can teach about health systems by discussing how our context impacts decisions.
*⃣Are all options equally feasible in our context?
*⃣What resources do we have available?
*⃣How much does each option cost?
It's also important to discuss equity (& inequity) explicitly.
*⃣Are all options equally feasible in our context?
*⃣What resources do we have available?
*⃣How much does each option cost?
It's also important to discuss equity (& inequity) explicitly.
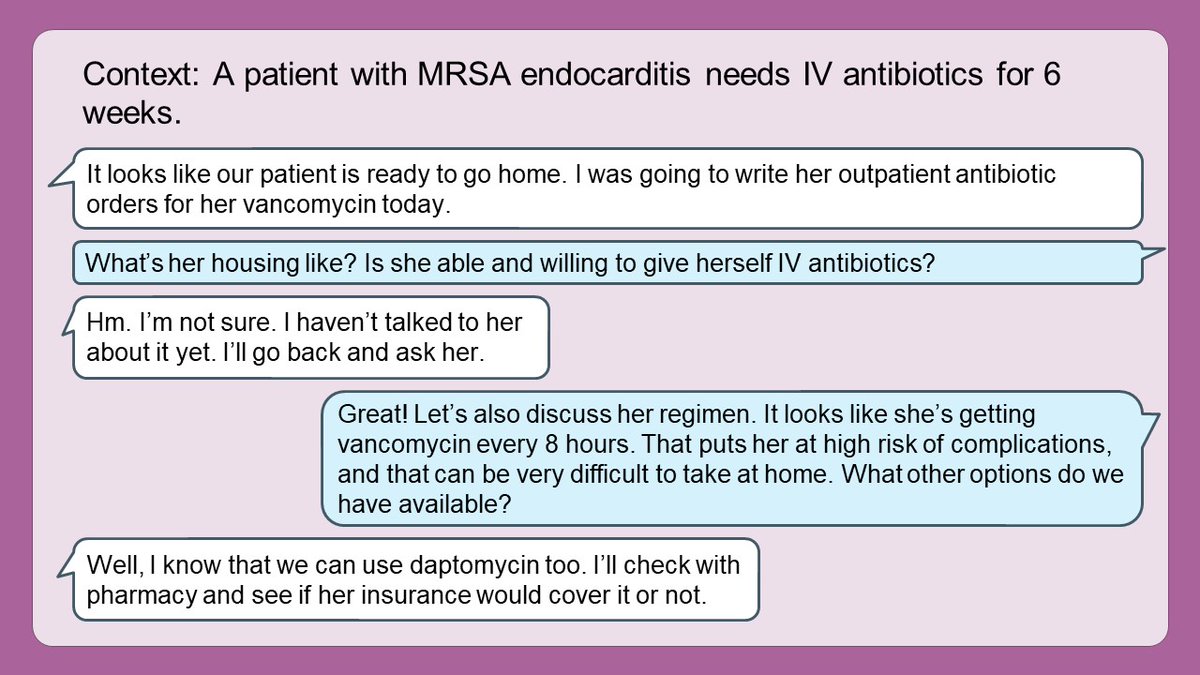
11/ Patient preferences are another important factor in management reasoning.
*⃣What are the patient's preferences regarding testing & treatment?
This is a great time to observe or role model discussions with patients.
*⃣What are the patient's preferences regarding testing & treatment?
This is a great time to observe or role model discussions with patients.
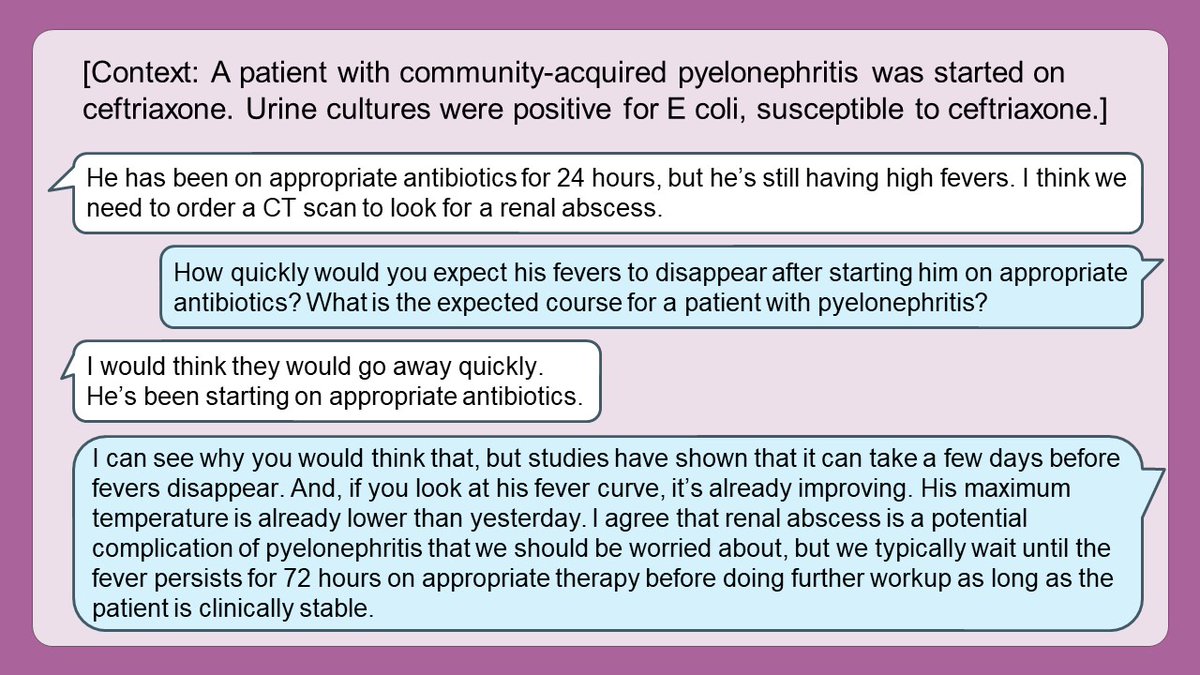
12/ Finally, it's important to teach learners what to EXPECT once treatment is started.
*⃣What's the typical time course for a response to treatment?
*⃣How will we know if the patient is improving?
*⃣What are the potential complications that could arise?
*⃣What's the typical time course for a response to treatment?
*⃣How will we know if the patient is improving?
*⃣What are the potential complications that could arise?
13/ Management reasoning is fun to teach because there's always more to teach & learn.
This is always a great time to engage specialists to help all of us refine our own management scripts. I know I take every opportunity to talk to other teams.
This is always a great time to engage specialists to help all of us refine our own management scripts. I know I take every opportunity to talk to other teams.
14/ But it's important to recognize that management reasoning can be frustrating, especially for early learners, because there isn't one right answer.
Uncertainty is uncomfortable. And hard.
Uncertainty is uncomfortable. And hard.
15/ Moreover, sometimes "style" drives decision-making, especially in evidence-sparse areas.
That's okay, but we should be upfront about this and explain our rationale.
Let's be good role models by avoiding absolutes and respecting others' opinions.
That's okay, but we should be upfront about this and explain our rationale.
Let's be good role models by avoiding absolutes and respecting others' opinions.
16/ In summary, here are some tools for teaching management reasoning.
Start with a management script for early learners, and then refine management reasoning by discussing more complex topics for more advanced learners.
Start with a management script for early learners, and then refine management reasoning by discussing more complex topics for more advanced learners.
17/ Join us next Tuesday when @GStetsonMD discussing asking effective questions to promote learning.
In the meantime, follow @MedEdTwagTeam, @YihanYangMD, & @ChrisDJacksonMD so that you don't miss any content!
In the meantime, follow @MedEdTwagTeam, @YihanYangMD, & @ChrisDJacksonMD so that you don't miss any content!
• • •
Missing some Tweet in this thread? You can try to
force a refresh