
Here is my summary of #fullerstocktake Report
Metaphorically speaking: It is written by management consultants for management consultants.
I shall elaborate more, as I walk through the report in this twitter thread.
Metaphorically speaking: It is written by management consultants for management consultants.
I shall elaborate more, as I walk through the report in this twitter thread.
My interpretation is, the report carries 20th century business ideology of "Globalisation is the key to profit"
NHS doesnt make profit as such, however, the working assumption of the report is - larger the scale, better the outcome
NHS doesnt make profit as such, however, the working assumption of the report is - larger the scale, better the outcome
The report has 21 Case Studies quoted various examples, some small, some slightly bigger. However, case studies are just that case studies.
It doesn't mean they can scale up! The report only shares positive bias, not a critical analysis on why PC Must Change?
It doesn't mean they can scale up! The report only shares positive bias, not a critical analysis on why PC Must Change?
Contract Model:
Scrap national GMS contract in favour of ICS led Primary Care Contract 👌
What else can we expect from an ICS CEO designate?
Scrap national GMS contract in favour of ICS led Primary Care Contract 👌
What else can we expect from an ICS CEO designate?

Urgent Care / Same day care!
This one is a particularly redundant concept. Have we not learnt from OOH services? How much additional work it has generated in primary care?
This one is a particularly redundant concept. Have we not learnt from OOH services? How much additional work it has generated in primary care?

This is akin to reincarnation of "Darzi Centres" Remember they were closed down for not providing VFM following similar review?
Do we need to unlearn and relearn the lessons again?
It doesnt work!
Same day appointment is a key data point to preventative care.
Do we need to unlearn and relearn the lessons again?
It doesnt work!
Same day appointment is a key data point to preventative care.
Remember the earlier tweet? Here is the recommendation. Hire a bunch of Management Consultant to "Hardwire Change"

Anyone with understanding of digital systems will realise how utterly painful the process this case study describes!

Hats off the team for making this model work.
But author should be asking,
1. Why e-Hub need to enter clinical info in community EPR?
2. Why report is sent as a DC document?
3. Have they quantified how much time EMIS takes to open DC Summary?
But author should be asking,
1. Why e-Hub need to enter clinical info in community EPR?
2. Why report is sent as a DC document?
3. Have they quantified how much time EMIS takes to open DC Summary?
It is not about 90% consultations were closed online the question is, how many of the 90% were actually needed?
Remember the report says "Data Data Data"
Again, thanks to frontline & sorry that the system has utterly failed to recognise the importance of this key metric
Remember the report says "Data Data Data"
Again, thanks to frontline & sorry that the system has utterly failed to recognise the importance of this key metric

The neighbourhood approach!
What is describes basically, PC take over all the responsbilities of secondary care, community services, social care.
Now, this is excellent as I have been advocating for long that GP Practices should provide wrap around all community care (not PCN!)
What is describes basically, PC take over all the responsbilities of secondary care, community services, social care.
Now, this is excellent as I have been advocating for long that GP Practices should provide wrap around all community care (not PCN!)
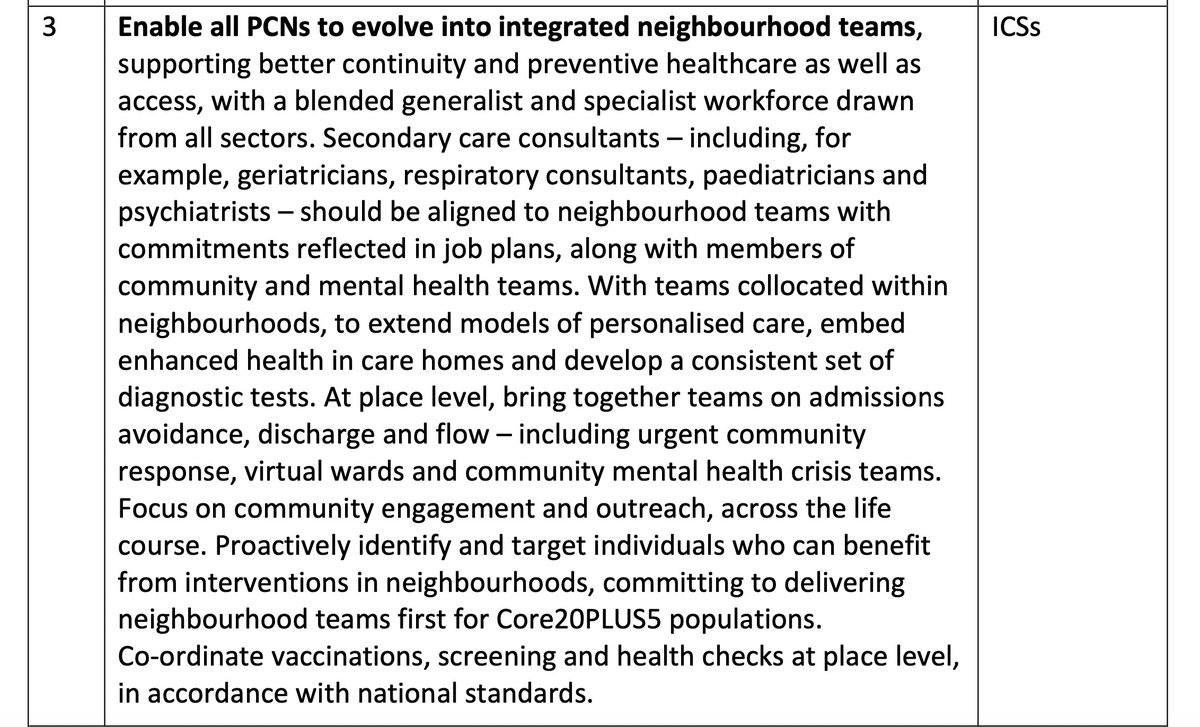
However, However, the report seems to assume that we have oversupply of Acute Physicians!!!
It would have been helpful if the report had actually quantified how many of such specialists are needed given we have >1000 PCN & how many are available. We cant even recruit ARRS!
It would have been helpful if the report had actually quantified how many of such specialists are needed given we have >1000 PCN & how many are available. We cant even recruit ARRS!
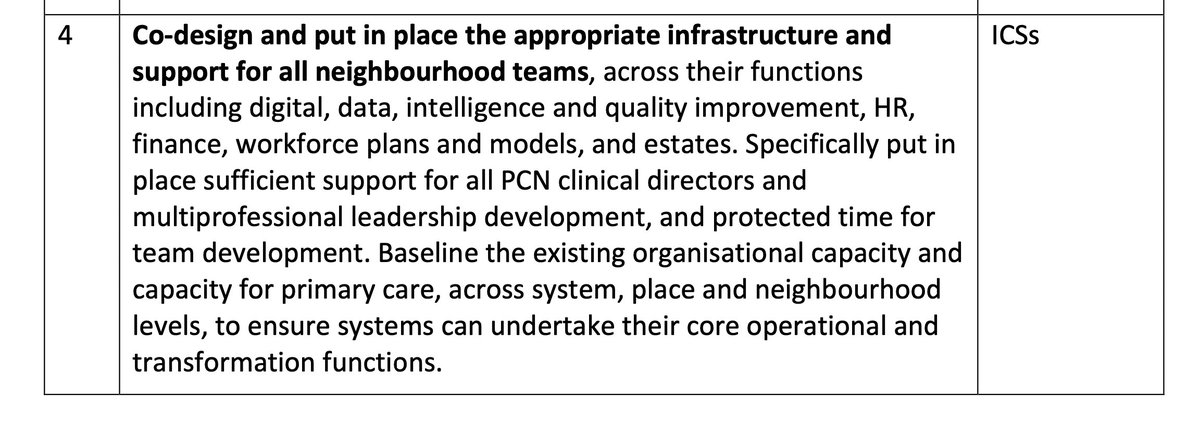
Next up: Infrastructure,
I thought the role of this report was to provide 👇If not what was the purpose - As a dive deep, I get even more perplexed
Remember my earlier tweet on Management Consultants? I assume they will get £££ to do 👇
I thought the role of this report was to provide 👇If not what was the purpose - As a dive deep, I get even more perplexed
Remember my earlier tweet on Management Consultants? I assume they will get £££ to do 👇
Let me ask, what is the so called "system thinking?"

There is ONE GP colleage on the ICS board, Just ONE!
Is the report proposing that >50% of the board is composed of colleages from PC / Community?
Is the report proposing that >50% of the board is composed of colleages from PC / Community?

This example of collective working is also biased. A densely populated small geographical footprint where CCG is now ICS is not similar in each region.
How will this model be implemented across other ICS more rural with multiple CCGs?
How will this model be implemented across other ICS more rural with multiple CCGs?

Finally,
I used an analogy of globalisation. This statement explains it all.
Where the world of business, technology etc is moving toward localisation following failed experimentation of globalisation.
Integrated Primary Care is trying to follow a failed model.
I used an analogy of globalisation. This statement explains it all.
Where the world of business, technology etc is moving toward localisation following failed experimentation of globalisation.
Integrated Primary Care is trying to follow a failed model.

In Summary,
The report is a missed opportunity that could have delivered substantial improvement to primary care.
It request resurrection of old failed experiments, uses case studies without critical analysis and summaries assumptions based on ideology not evidence.
The report is a missed opportunity that could have delivered substantial improvement to primary care.
It request resurrection of old failed experiments, uses case studies without critical analysis and summaries assumptions based on ideology not evidence.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



