
Our Pre-print on exhaled breath detection of COVID-19 and bacteria from your lung. TL;DR summary: you do not emit any virus if you are infected, have symptoms, and are breathing in a relaxed fashion.
This DOES NOT mean COVID-19 isn’t airborne 1/n medrxiv.org/content/10.110…
This DOES NOT mean COVID-19 isn’t airborne 1/n medrxiv.org/content/10.110…
People emit a lot more aeorosols in different ways when they talk, shout, sing, etc. Please wear a mask because we have 3 new variants with more disease burden poised to make our collective summers a mess.
We are working to find out how much virus you emit otherwise 2/n
We are working to find out how much virus you emit otherwise 2/n
This starts with a student wanting to test living under bridges with tuberculosis. At the time (2012) pretty much every breath collector out there was considered contaminated, so we set out to solve contamination, sample loss, reproducibility erj.ersjournals.com/content/26/3/5… 3/n
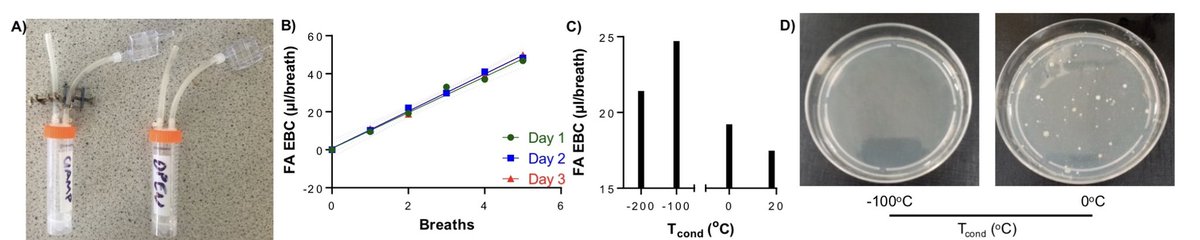
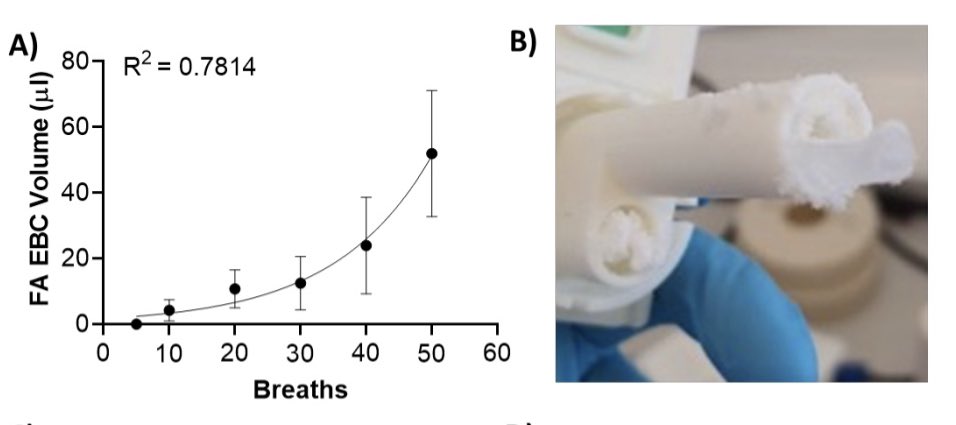
So we built these. A common lab vial attached to low adhesion tubes, clamped to prevent contamination/sample loss, and with a 10 cent saliva trap- an inertial impactor for large droplets. Dunk these in ice, and presto: you can condense breath pretty efficiently 4/n 

Efficiently and reproducibly. As you can see the breath sample increases linearly for the number of breaths, doesn’t change day to day. It works better with dry ice instead or crushed ice, and kills the bacteria in the breath sample in the process (safer to use). 5/n
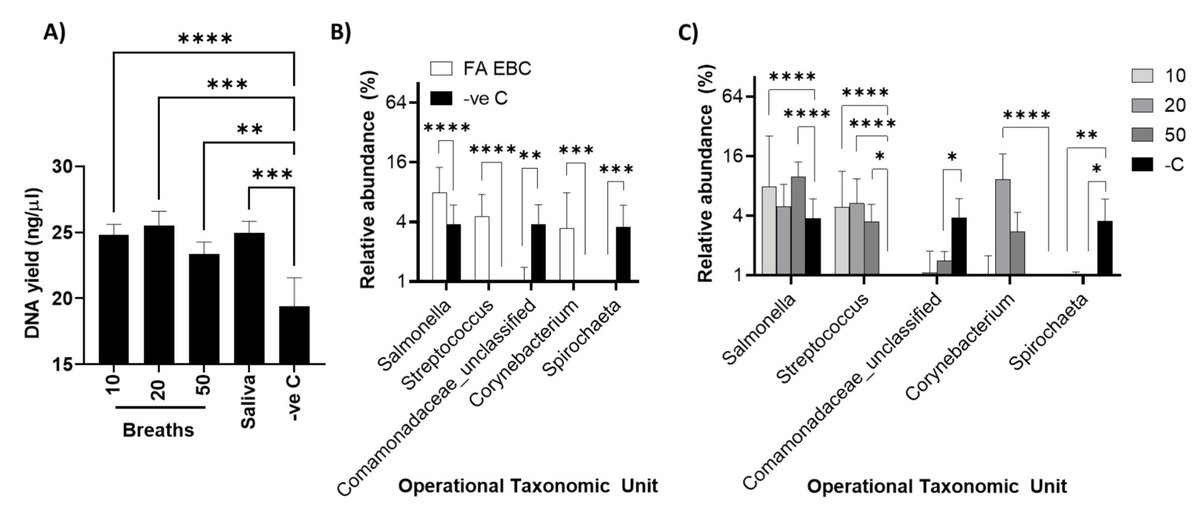
But what was eye popping was the microbiota data. NONE of the bacterial DNA in the breath sample proper was found in the saliva trap DNA. Importantly we amplified the DNA directly from the samples, not after extraction, because of contamination in the extraction kits. 6/n

We did this in March 2014. Later on @pathogenomenick and others coined the term kitome contaminants- but we used the exact same method during the EbolaCheck project in autumn 2014 for Ebola virus RNA in blood pubs.rsc.org/en/content/art… 7/n
What I’d learnt from EbolaCheck was that nobody would talk to you if an ISO- accredited company wasn’t behind the medical device or diagnostic. So with @Northern_Acc and @innovateuk #icure support @PulmoBioMed was born to make PBM-HALE to help diagnose paediatric wheeze 8/n
Then the pandemic hit. On 24/1/20 I set out to find out if SARS-CoV-2 can be found in exhaled breath, starting with York 2 in the Newcastle RVI HCID and like many others later, was dismissed, even ridiculed. bbc.com/news/uk-englan… 9/n
In the meantime we went to first principles. We showed our breath collector linearly collected samples between 0.5-30 min. It did this by rapidly (2 sec) freezing (> -80) fine aerosols whilst the person being sampled inhaled. In doing so, the fine aerosols inside swelled up. 10/n

This video shows the freezing of the tidal breath during inhalation much better than the stills. medrxiv.org/content/medrxi… 11/n
The figures on particle size show how freezing temperature (X axis) alters particle count (Y axis), for different size particles (each graph is a different size. As condensing temperature drops, particles swell more. More gas water condenses on the particles (dry or wet) 12/n
We confirmed these breath condensates contained bacteria which lost viability at low condensation temperature. We confirmed there is not a smidgeon of saliva in the breath sample- tried over 300 times now. At worst, for every 1,750 parts of breath, there’s 1 part saliva. 13/n
Besides (bacterial) DNA, we found RNA, a tiny amount of protein, and metabolites: no metabolites were detected UNLESS we extracted the sample. This means cells or exosomes. The known metabolites were largely membrane compounds, and even a cocaine metabolite. 14/n
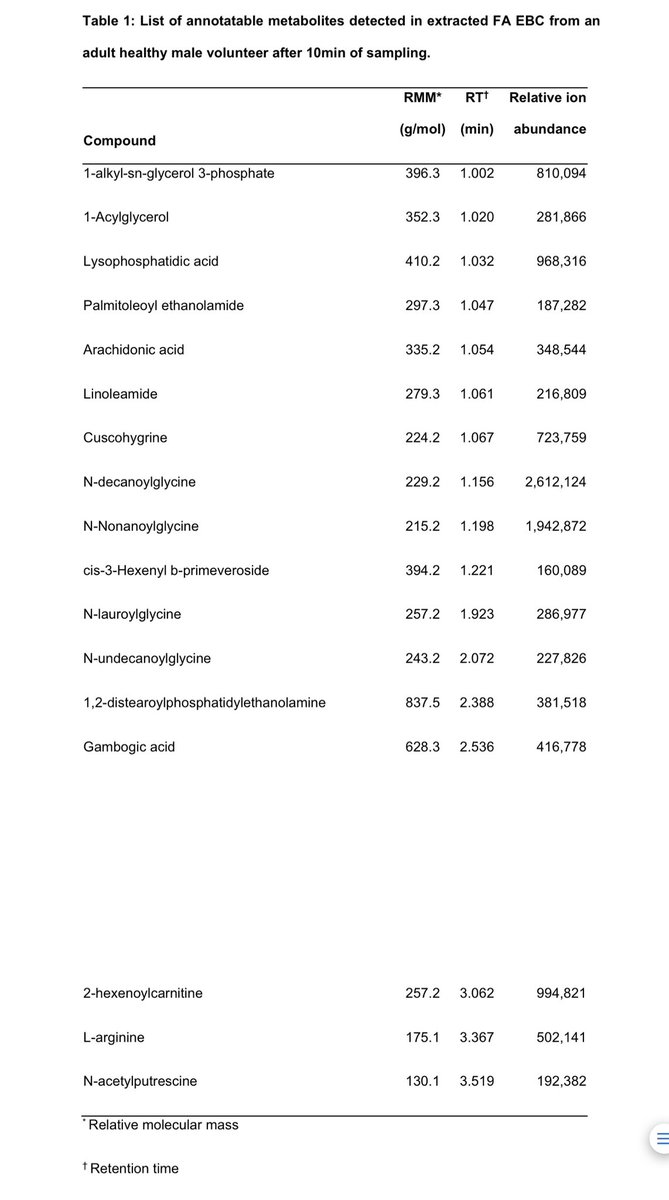
The presence of cuscohygrine and absence of soluble metabolites is unique to our device. Previous reports with other devices show soluble metabolites, or cocaine. Cuscohygrine is absent from saliva. Those devices suffer saliva contamination. 14/n pubmed.ncbi.nlm.nih.gov/30395206/
The participant had reported use of cocaine by inhalation 2.5 days before offering a breath sample. For us the salivary amylase activity, cuscohygrine, and microbiota data suggests the breath sample is very pure if not entirely devoid of saliva. This matters for 🦠 emission 15/n
and understanding where the virus comes from. So @ewrightlab gave us some pseudotyped lentivirus encoding GFP to nebulise and capture with PBM-HALE. The device captured the virus, which retained infectivity. @uni_ulm validated this with VLPs. Charge aggregates particles. 16/n


At this point we fully anticipated if SARS-CoV-2 was in exhaled breath, we would see it by RT-PCR. PLOT TWIST: We found none, among 42 cases, 30 of which in days 0-5 from start of symptoms sampled Aug 21-Jan 22, with a limit of detection of 4.7 genomes per min breathing. 17/n
This equates to <120 virus 🦠 genomes per mL of breath condensate. The average vol of breath condensate produced was 1.18 mL and we analysed 0.2 mL after adding a spike in control into the condensate. This was fully detected by RT-PCR. 18/n
There is not a single molecule of SARS-CoV-2 RNA in exhaled breath, dead or alive, n=42. The lowest nasopharyngeal swab Ct in these participants was 13.1. Ridiculous levels of infection. We used CDC swabbing guidelines BTW. 19/n
This is where I had to think long and hard and very responsibly about this data. I communicated to key individuals, such as @ArisKatzourakis. There is nuance in these data that the press would miss in August ‘21. Why were we not finding SARS-CoV-2? 20/n
We had one member of the team pick up a cold. They were SARS-CoV-2 free by NP swab. We tested their breath condensate for microbial DNA and @nuomics @andrewnelsonphd used modern data processing methods across samples. Streptococcus. 21/n
Did we lyse the virus by swelling the aerosols with molecular water, creating osmotic shock and RNase exposure? -100oC condensation increases condensate vol 13.9x, but the protein drops only 2.2x. We’re pulling dry breath particles into the condenser, not diluting. 22/n
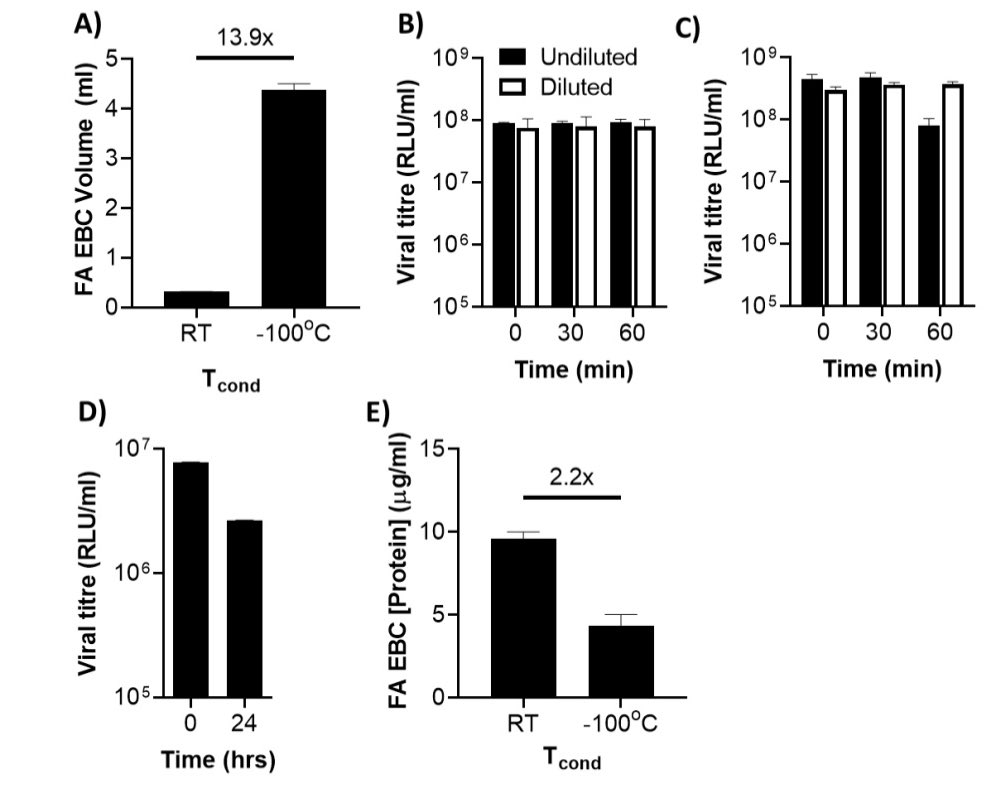
Lentivirus, which is also an enveloped lentivirus, can actually shrug off dilution with 18.5 MegaOhm water and freezing. We are not therefore destroying SARS-CoV-2 viruses or their RNA: it’s simply not there. Does this mean COVID19 is not airborne? NO 23/n
To measure virus in our device’s large droplets inertial impactor you need to break into it. We didn’t have the luxury of doing this with 3D printed devices; the ones we broke showed saliva (diluted a bit) in the large droplets fraction medrxiv.org/content/medrxi… 24/n
We know there is SARS-CoV-2 in saliva as @VirusesImmunity showed. @linseymarr @Don_Milton @jljcolorado @CathNoakes @trishgreenhalgh and Lydia Bourouiba among many others have explained why and how they become airborne. 25/n
We also didn’t sample talking, singing, or shouting. @Don_Milton & @drkristenkc have shown it’s much more likely this increases 🦠 emissions- but we still can’t say where it’s coming from: the lungs, or the mouth? 26/n
Many others have tried similar studies: breath-based detection rates range 0-93% for positive cases, but the devices either don’t separate saliva, or allow too much space for the exhaled breath particles to evolve in size. The environmental conditions will affect this. 27/n
The one device with zero detection in tidal breath, like ours, used a 35L box fitted with a pump at the top to pick up fine aerosols. No virus. When they used a downward tube that could get contaminated with saliva, samples were positive. 28/n
What are the implications to society? Based on the current data, you will prevent infecting others if you wear a face covering when speaking, laughing singing, etc. If you’re keeping quiet, you are safe to others. Let’s face it, nobody stays permanently stone faced, so 😷👍
What does it mean for respiratory research? We found it incredibly easy to break the ‘magic sauce’ preventing saliva contamination, sampling linearity or device blockage. Others tried CFD-designed EBC collection & still had saliva contamination 29/n ncbi.nlm.nih.gov/pmc/articles/P…
We hope that our solution can now help separate signals from the deep lung as opposed to stuff with saliva contamination and open up the biomarker/diagnostics to other analytes beyond volatiles for clinical use in any of the 40-odd diseases with associated breath biomarkers 30/n
In a future thread, I will explain in detail why other devices out there give such conflicting data on aerosol load of the virus. Let’s hope BA.4, BA.5, B2.1.12 or monkeypox and their followers don’t make us have to consider breath screening in the future. Please use 😷 💉.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


