#ASCO22
✳️Happy to say there is great progress for patients with CRC‼️
@OncoAlert @ASCO @manjuggm @CrcChange‼️
Here is summary of some key studies 👇
✳️Happy to say there is great progress for patients with CRC‼️
@OncoAlert @ASCO @manjuggm @CrcChange‼️
Here is summary of some key studies 👇
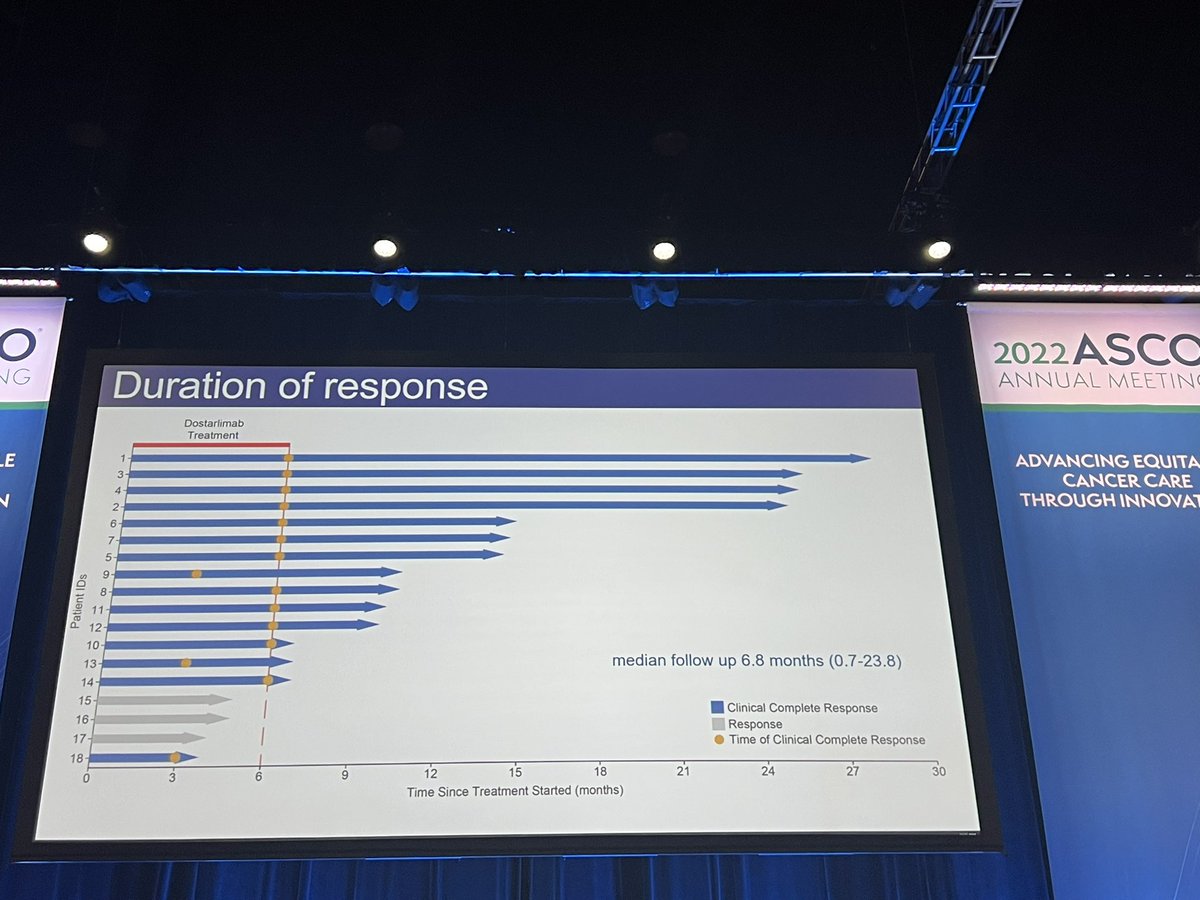
1️⃣ Immune checkpoint inhibitor monothetapy with dostarlimab for MMR-D is certainly practice changing❗️
✳️Although long term outcomes are needed, no need to reinvent the wheel‼️
✳️ Once a deep response achieved in MMR-D CRC it is very durable even in metastatic setting ‼️
✳️Although long term outcomes are needed, no need to reinvent the wheel‼️
✳️ Once a deep response achieved in MMR-D CRC it is very durable even in metastatic setting ‼️

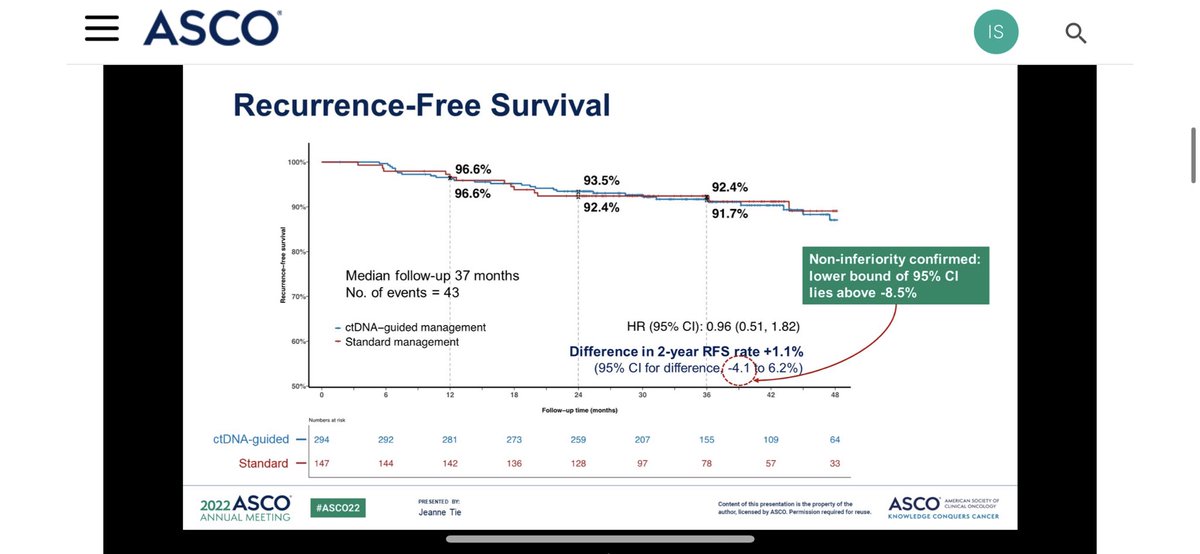
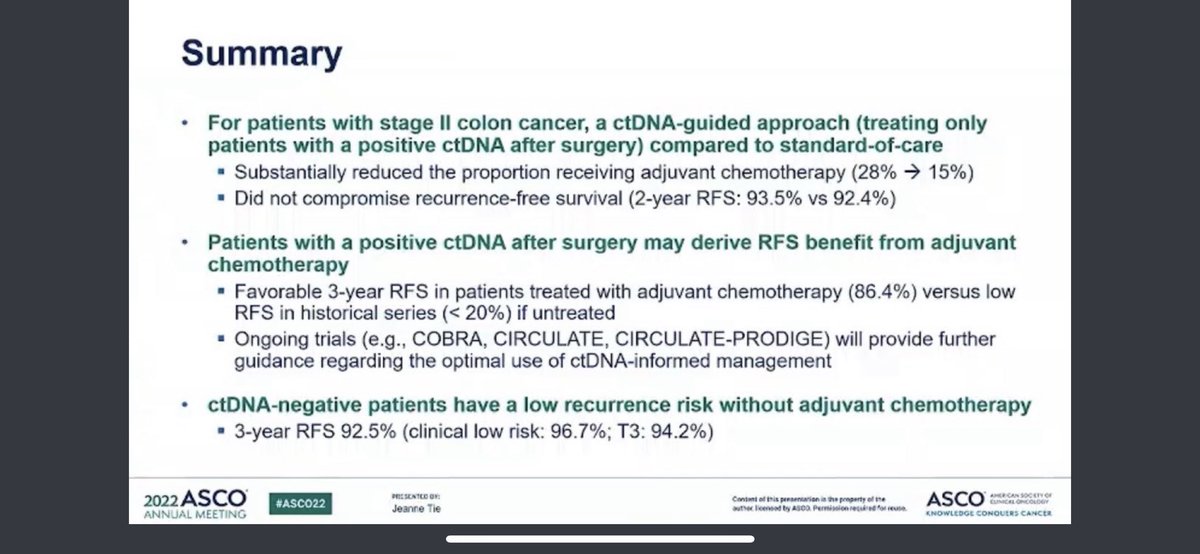
2️⃣ #ctDNA study (DYNAMIC) was my second favorite study ❗️
✳️ We are certainly in the right pathway to use #ctDNA however we have to be careful for false negative results in high risk population: T4 disease ‼️
✳️We need more trials to get more data ❗️Enroll COBRA/CIRCULATE
✳️ We are certainly in the right pathway to use #ctDNA however we have to be careful for false negative results in high risk population: T4 disease ‼️
✳️We need more trials to get more data ❗️Enroll COBRA/CIRCULATE

3️⃣ NICHE trial is quite provocative and highly exciting for MSI-H and perhaps somewhat promising for MSS colon❗️
✳️A downside of the study to identify right population to treat in neoadjuvant setting ! Radiological staging has not been well established for colon cancer ‼️
✳️A downside of the study to identify right population to treat in neoadjuvant setting ! Radiological staging has not been well established for colon cancer ‼️

4️⃣ For example, do we really need IO for patient with N(-) and/or T3 know IRAEs❓Where ctDNA settles in?
✳️if WW is considered as evolving approach, then cCR for colon cancer is not well established unlike rectal‼️
✳️ Also we need to keep our CR surgeons in business ☺️
✳️if WW is considered as evolving approach, then cCR for colon cancer is not well established unlike rectal‼️
✳️ Also we need to keep our CR surgeons in business ☺️
5️⃣ 29% Major response (not all cCR) in MSS is nice but we have to acknowledge even metastatic setting chemotherapy has higher response rate ‼️
✳️ Nonetheless seeing some response with IO alone for pts with MSS is exciting and warrants more correlative ❗️
✳️ Nonetheless seeing some response with IO alone for pts with MSS is exciting and warrants more correlative ❗️
6️⃣NIVACOR Trial investigated the chemoimmunotherapy and maintenance bev+IO combination for pts with nCRC❗️
✳️ Single arm study and inclusion of pts with MSI-H CrC makes it hard to evaluate the additive role of IO ‼️
✳️It is time to separate trials for MSI-H/MSS (actually due)❗️
✳️ Single arm study and inclusion of pts with MSI-H CrC makes it hard to evaluate the additive role of IO ‼️
✳️It is time to separate trials for MSI-H/MSS (actually due)❗️
7️⃣More and more studies investigating the nonoperative approach for rectal cancer ❗️
✳️New XRT modalities and dosing seem to be on improving organ preservation‼️
✳️Glad there is consensus in enthusiasm on this pathway ❗️
✳️New XRT modalities and dosing seem to be on improving organ preservation‼️
✳️Glad there is consensus in enthusiasm on this pathway ❗️
8️⃣Clonal evolution of colorectal cancer allows to rechallenge EGFR responsive therapies as long as downstream mutations (RAS/RAF) does not occur‼️
✳️EGFR rechallenge trials are quite relevant and exciting to see the interest is continuing to evolve!
✳️EGFR rechallenge trials are quite relevant and exciting to see the interest is continuing to evolve!
9️⃣ The PARADIGM trial remonstrated what FIRE-3 trial ! No practice changing rather confirming ‼️
✳️Left sided CRC responds better EGFR blockadeand can be considered as first biologic agent in combination with chemotherapy
✳️Left sided CRC responds better EGFR blockadeand can be considered as first biologic agent in combination with chemotherapy
1️⃣0️⃣ The Optical trial is important❗️
✳️This study looked into perioperative chemotherapy DID not improve DFS‼️
✳️I get worried about correct clinical staging of colon cancer in locally advance setting unlike rectal cancer. Overtreatment vs Undertreatment (with CIRCULATE-US)
✳️This study looked into perioperative chemotherapy DID not improve DFS‼️
✳️I get worried about correct clinical staging of colon cancer in locally advance setting unlike rectal cancer. Overtreatment vs Undertreatment (with CIRCULATE-US)
1️⃣1️⃣The IMPROVE trial offers an approach with intermittent use EGFR blockade to avoid toxicity and decrease resistance‼️
✳️I think this is relevant for toxicity (increase compliance) but not sure this addresses resistance perhaps changes the course of clonal evolution ❗️
✳️I think this is relevant for toxicity (increase compliance) but not sure this addresses resistance perhaps changes the course of clonal evolution ❗️
1️⃣2️⃣ Conflicting results with Bevacizumab versus Anti-EGFR containing triplet regimens‼️
✳️We know bevacizumab works better with triplet mostly due to toxicity of anti-EGFR with triplet may become overwhelming (rash/diarrhea:fatigue)!
✳️We know bevacizumab works better with triplet mostly due to toxicity of anti-EGFR with triplet may become overwhelming (rash/diarrhea:fatigue)!
1️⃣3️⃣One thing I believe causing confusion clinical trial inclusion criteria and inclusion of pts with right sided colon cancer ‼️
✳️Nonetheless, as of now, bevacizumab seems be a better companion for triplet chemotherapy ‼️
✳️We need more studies with clearer designs❗️
✳️Nonetheless, as of now, bevacizumab seems be a better companion for triplet chemotherapy ‼️
✳️We need more studies with clearer designs❗️
1️⃣4️⃣ Perhaps there are so many other exciting studies could not include here, But the progress in #ASCO22 for pts with CRC is very encouraging and I am happy to see that for our patients‼️
✳️That being said there is significant unmet need for precision medicine and immunotherapy
✳️That being said there is significant unmet need for precision medicine and immunotherapy
1️⃣5️⃣An add on (recognized that I missed that important one)‼️
✳️Removing primary for pts with unresectable metastatic disease do no benefit and should be avoided as this approach delays initiation of systemic therapy ‼️
✳️Removing primary for pts with unresectable metastatic disease do no benefit and should be avoided as this approach delays initiation of systemic therapy ‼️
• • •
Missing some Tweet in this thread? You can try to
force a refresh