A short thread on the revised list of AGPs
The AGP list has changed in England
The following are no longer considered to be AGPs
@TonyPi314 @_andyshrimp @drjulesbrown @NWilson247 @EuanTovey
1/6
The AGP list has changed in England
The following are no longer considered to be AGPs
@TonyPi314 @_andyshrimp @drjulesbrown @NWilson247 @EuanTovey
1/6

These changes are laid out in the new NHS National IPC manual (14 April 2022)
england.nhs.uk/wp-content/upl…
2/6
england.nhs.uk/wp-content/upl…
2/6
The evidence review that underpins this change in AGPs is now published here (9 June 2022).
Clinical guidance on this review was provided by the #AERATOR anaesthesia group amongst others
england.nhs.uk/wp-content/upl…
4/6
Clinical guidance on this review was provided by the #AERATOR anaesthesia group amongst others
england.nhs.uk/wp-content/upl…
4/6
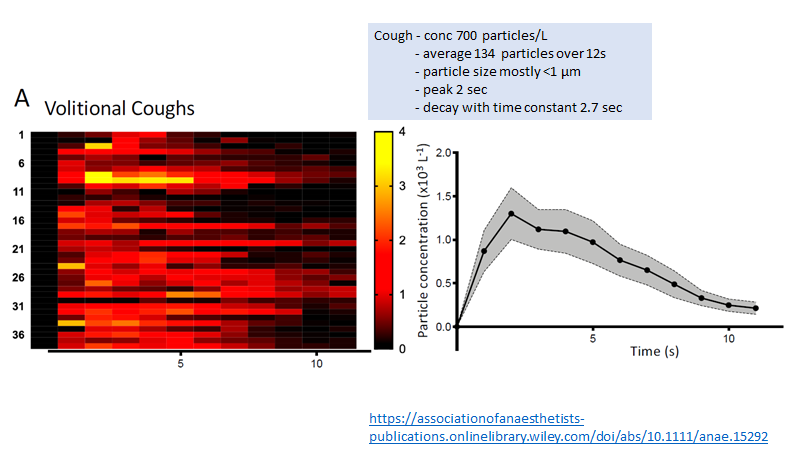
Of note the remit of this review was only to explore removal of procedures from the AGP list.
The same studies that show procedures not producing aerosols show aerosol generation by exertional respiratory activity
Eg …-publications.onlinelibrary.wiley.com/doi/10.1111/an…
…-publications.onlinelibrary.wiley.com/doi/10.1111/an…
5/6
The same studies that show procedures not producing aerosols show aerosol generation by exertional respiratory activity
Eg …-publications.onlinelibrary.wiley.com/doi/10.1111/an…
…-publications.onlinelibrary.wiley.com/doi/10.1111/an…
5/6


So… the AGP list is now appropriately reduced
RISK assessment is still required & should be based around patient, context, mitigation & consequences of infection
thelancet.com/journals/lanre…
6/6
RISK assessment is still required & should be based around patient, context, mitigation & consequences of infection
thelancet.com/journals/lanre…
6/6


• • •
Missing some Tweet in this thread? You can try to
force a refresh