
Yet another large trial of ivermectin is now complete & the results are negative.
ACTIV-6 found no difference in mortality or hospitalization when people with COVID were randomized to ivermectin.
Yet another nail in the ivermectin ⚰️
Preprint medrxiv.org/content/10.110…
1/
ACTIV-6 found no difference in mortality or hospitalization when people with COVID were randomized to ivermectin.
Yet another nail in the ivermectin ⚰️
Preprint medrxiv.org/content/10.110…
1/


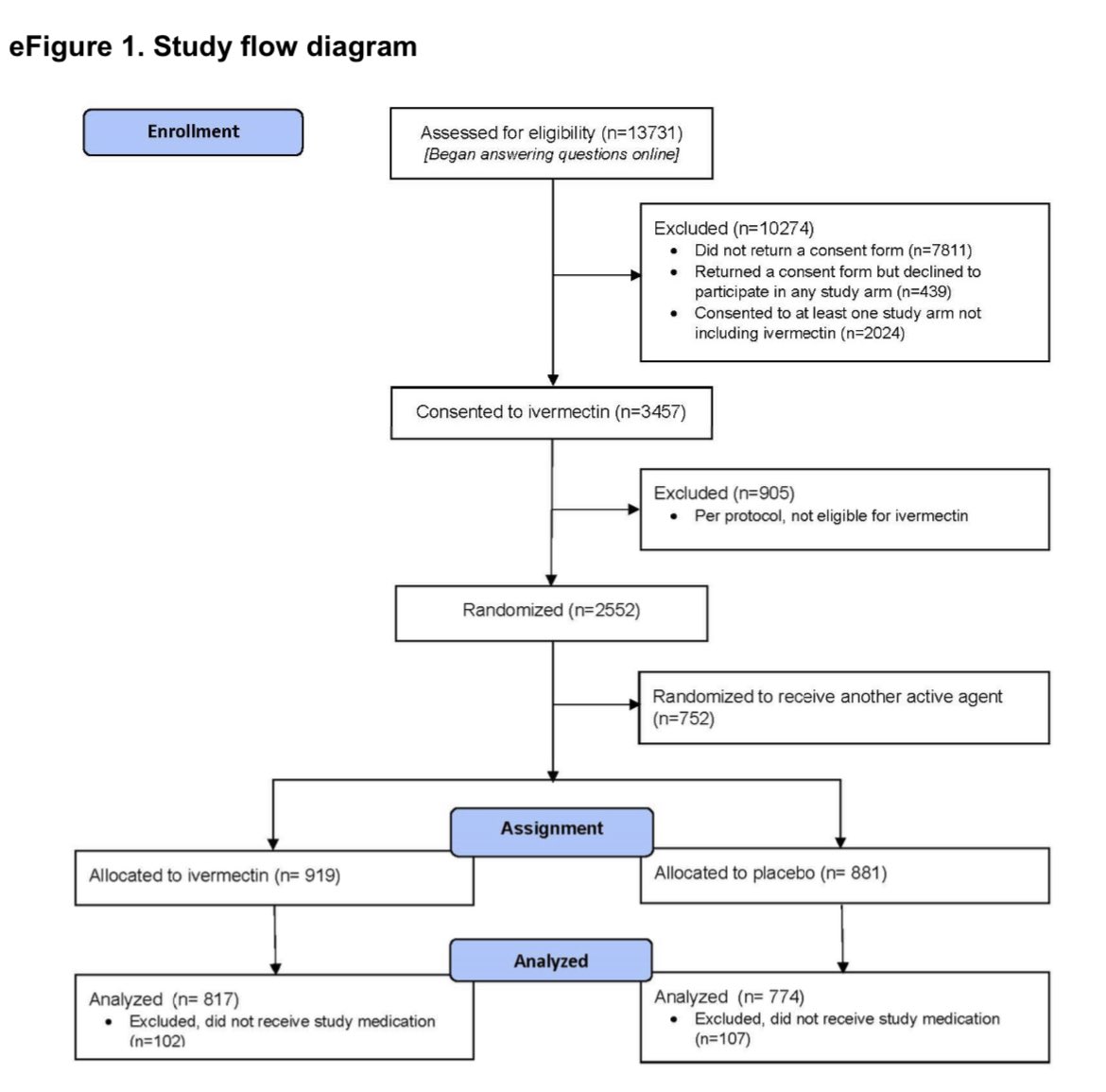
ACTIV6 is a large placebo controlled RCT performed at 93 sites in the 🇺🇸 by @DCRINews
It enrolled adults >30yo w symptomatic COVID. They were randomized to either ivermectin or placebo.
The primary endpoints were death, Hospitalization, & symptoms
clinicaltrials.gov/ct2/show/NCT04…
2/
It enrolled adults >30yo w symptomatic COVID. They were randomized to either ivermectin or placebo.
The primary endpoints were death, Hospitalization, & symptoms
clinicaltrials.gov/ct2/show/NCT04…
2/
It was a “fully decentralized study”, meaning patients could be enrolled remotely & medication shipped to their home (via next day mail). Follow up was either remote or in person.
Theoretically this is a great pragmatic way to enroll a large number of people in a trial.
3/
Theoretically this is a great pragmatic way to enroll a large number of people in a trial.
3/
The trial has multiple arms & tested multiple doses of ivermectin:
- Low dose was 400 mcg/kg x 3 days (this is what was just published as a pre-print)
- High dose was 600 mcg/kg x 6 days (this is definitely a high dose; it is still ongoing)
4/
- Low dose was 400 mcg/kg x 3 days (this is what was just published as a pre-print)
- High dose was 600 mcg/kg x 6 days (this is definitely a high dose; it is still ongoing)
4/
The study enrolled n=1559, and n=817 were assigned to ivermectin and n=774 to placebo.
The patients had a median age of 47 yo, with the typical comorbidities.
~1/2 were unvaccinated & 1/2 had received 2 or more vaccine doses.
Median time from symptom onset to tx was 6 days
5/
The patients had a median age of 47 yo, with the typical comorbidities.
~1/2 were unvaccinated & 1/2 had received 2 or more vaccine doses.
Median time from symptom onset to tx was 6 days
5/

The results were stone cold negative.
People treated with ivermectin had no decrease in hospitalization or mortality. The event rate was very low however; only one death occurred in the study, which was in the ivermectin arm.
6/
People treated with ivermectin had no decrease in hospitalization or mortality. The event rate was very low however; only one death occurred in the study, which was in the ivermectin arm.
6/


What’s with the low event rates?
3-4% rates of hospitalization or ED visit certainly are lower than we’ve seen in most studies. (Compare to the EPIC-HR study of paxlovid)
But recall that ACTIV6 didn’t enroll only high risk patients & and it did enroll vaccinated people.
7/
3-4% rates of hospitalization or ED visit certainly are lower than we’ve seen in most studies. (Compare to the EPIC-HR study of paxlovid)
But recall that ACTIV6 didn’t enroll only high risk patients & and it did enroll vaccinated people.
7/
https://twitter.com/nickmmark/status/1456683442825928707
Time to symptom resolution (or conversely mean time unwell) was not clinically or statistically different: 10.96 days vs 11.45 days.
Even with the most optimistic priors the likelihood that ivermectin shortens symptoms by even one day is <1%.
8/
Even with the most optimistic priors the likelihood that ivermectin shortens symptoms by even one day is <1%.
8/


Fortunately at this dose (400 mcg/kg x3 days) there were few adverse effects. So while ivermectin does not appear to be doing anything beneficial at least it isn’t harmful.
(It will be interesting to see what the AEs look like at a higher dose given for longer).
9/
(It will be interesting to see what the AEs look like at a higher dose given for longer).
9/
So what can we conclude from this?
In a large randomized double blind placebo controlled study performed in the US, ivermectin failed to demonstrate *any* significant clinical benefit.
Like *every* high quality RCT (I-TECH, EPIC, IVERCORCOVID, TOGETHER) this was negative.
10/
In a large randomized double blind placebo controlled study performed in the US, ivermectin failed to demonstrate *any* significant clinical benefit.
Like *every* high quality RCT (I-TECH, EPIC, IVERCORCOVID, TOGETHER) this was negative.
10/
I’m sure the usual crowd of ivermectin zealots will opine, so let’s try to anticipate & respond to their criticisms:
11/
11/
“ThE dOsE wAs ToOoO Low!”
This was the same dose proponents claimed was effective back in 2020 & 2021.
RCTs using a higher dose have also been negative (see I-TECH). Another arm of ACTIV6 is looking at 600 mcg/kg x 6 days. I’m not holding my breath that it will be different
12/
This was the same dose proponents claimed was effective back in 2020 & 2021.
RCTs using a higher dose have also been negative (see I-TECH). Another arm of ACTIV6 is looking at 600 mcg/kg x 6 days. I’m not holding my breath that it will be different
12/
https://twitter.com/nickmmark/status/1455888984932978693
“ThEy StArTeD tReAtMeNt ToOoO late”
The median was 6 days after symptom onset. This seems like a long time to wait for “early therapy.” However if we look at the subgroup who got treatment earlier (within 3 days of onset) they did… no better than those at 5, 7, or 9 days.
13/
The median was 6 days after symptom onset. This seems like a long time to wait for “early therapy.” However if we look at the subgroup who got treatment earlier (within 3 days of onset) they did… no better than those at 5, 7, or 9 days.
13/

“WhAt aBoUt UTTAR PRADESH!?”
The UP narrative has been pretty thoroughly debunked. The COVID stats from UP are dubious; entire districts show no deaths from *ANY* cause for months. Either IVM literally prevents death from EVERYTHING or the data is 🗑
onepagericu.com/blog/debunking…
14/
The UP narrative has been pretty thoroughly debunked. The COVID stats from UP are dubious; entire districts show no deaths from *ANY* cause for months. Either IVM literally prevents death from EVERYTHING or the data is 🗑
onepagericu.com/blog/debunking…
14/

“ThIs StUdY iS fAaAke!”
I see no evidence of any glaring errors but I’m curious to see what peer reviewers find.
Notably the #CultOfIvermectin accuses any negative study of being fake but still haven’t admitted that Elegazzar & others actually were. It’s been a year…
15/
I see no evidence of any glaring errors but I’m curious to see what peer reviewers find.
Notably the #CultOfIvermectin accuses any negative study of being fake but still haven’t admitted that Elegazzar & others actually were. It’s been a year…
15/


“Why are we still talking about this?”
Good question!
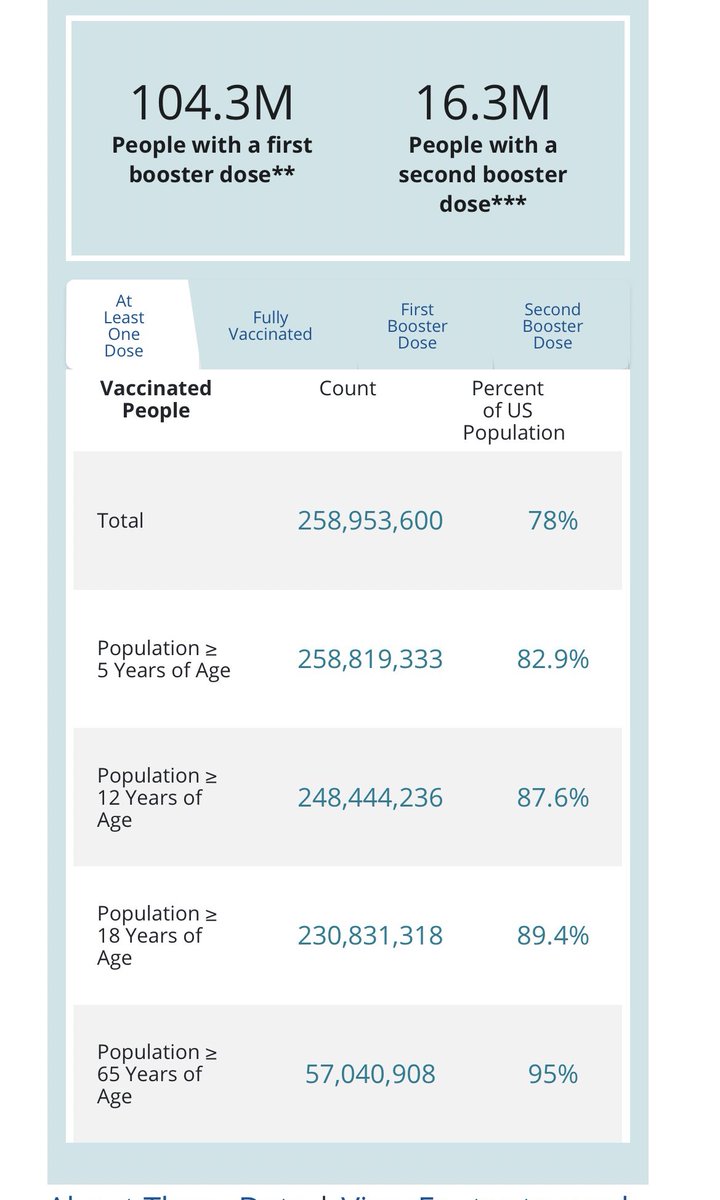
Most of the US is vaxxed; ~90% adults have had ≥1 shot. Most peoples interest in ivermectin is waning
But with many cults, as more is disproved, the more zealously the #CultOfIvermectin believes
16/
Good question!
Most of the US is vaxxed; ~90% adults have had ≥1 shot. Most peoples interest in ivermectin is waning
But with many cults, as more is disproved, the more zealously the #CultOfIvermectin believes
https://twitter.com/nickmmark/status/1430671783632330753?s=21
16/

I started debunking ivermectin because I was tired of watching people taking it die of COVID in my ICU.
No amount of high quality studies will ever convince the high priests & priestesses of ivermectin. But perhaps a few more of their vulnerable followers can be saved.
17/17
No amount of high quality studies will ever convince the high priests & priestesses of ivermectin. But perhaps a few more of their vulnerable followers can be saved.
17/17

• • •
Missing some Tweet in this thread? You can try to
force a refresh































