Today's 🧵is on the Gigli saw:
Some of its uses, how to use it, and a little of its history (including its obstetric origin), and the sad fate of Leonardo Gigli.
Some of its uses, how to use it, and a little of its history (including its obstetric origin), and the sad fate of Leonardo Gigli.

The Gigli saw is not complicated. It's a wire saw and two handles.
The wire is passed around the bone, and the saw is drawn back and forth, usually with the hands at (roughly) a 90 degree angle.
For larger bones, irrigation can be done to minimize heat from friction.
The wire is passed around the bone, and the saw is drawn back and forth, usually with the hands at (roughly) a 90 degree angle.
For larger bones, irrigation can be done to minimize heat from friction.

It has been used for craniotomies (though less common today).
Burr holes are made, and then the saw is used to 'connect the dots'.
This requires specialized wire passing devices and modifications to the blade, which are beyond our scope here. See Brunori et al (1995) for more.
Burr holes are made, and then the saw is used to 'connect the dots'.
This requires specialized wire passing devices and modifications to the blade, which are beyond our scope here. See Brunori et al (1995) for more.

When necessary, the Gigli saw may be used for almost any extremity amputation in place of a powered saw.
It may be preferred for certain foot and ankle amputations and (apparently) revisional hip surgery.
It may be preferred for certain foot and ankle amputations and (apparently) revisional hip surgery.

Historically, it has been used in a number of different head and neck resections, as seen in these old diagrams.
I am not sure if it is still used in head and neck surgery, so if anyone wants to chime in, that would be great.
I am not sure if it is still used in head and neck surgery, so if anyone wants to chime in, that would be great.


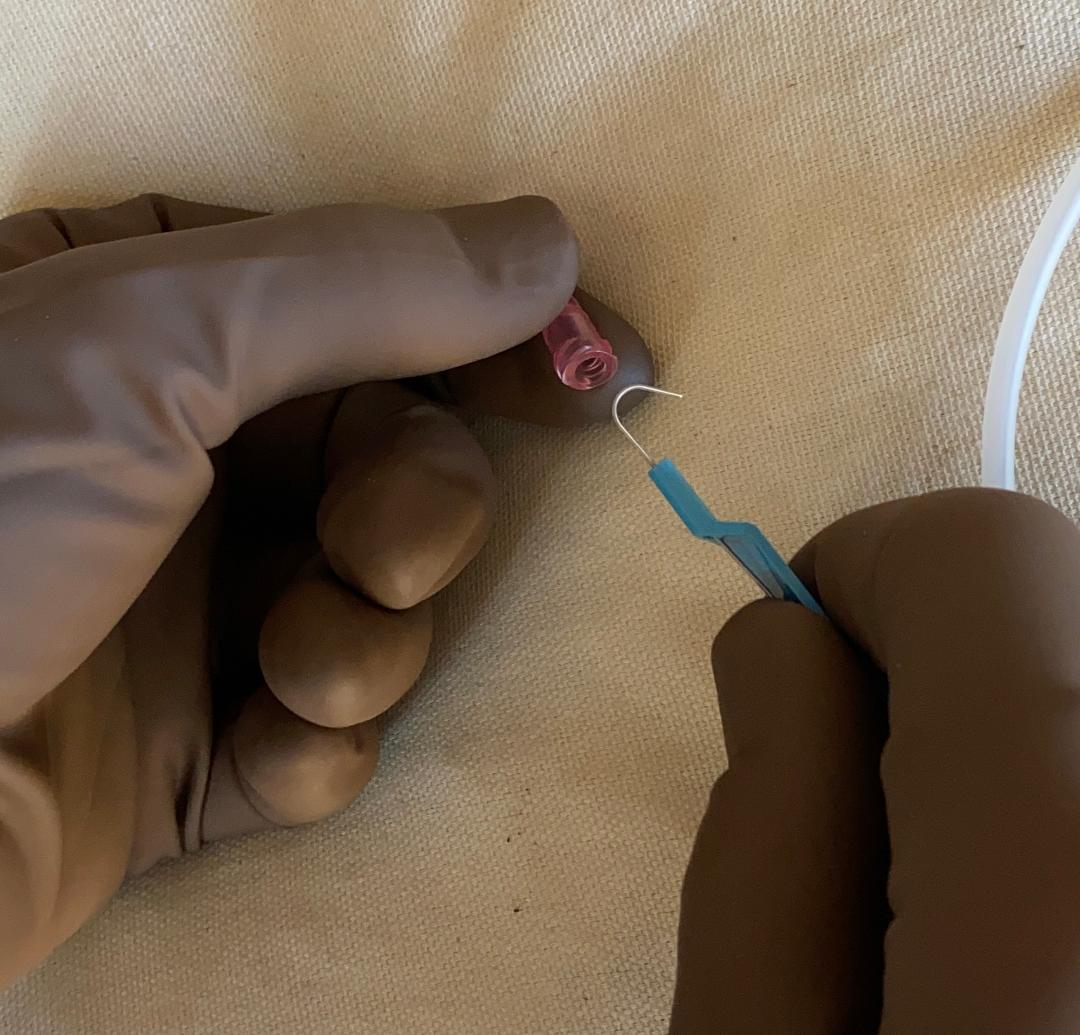
This is a closeup of a modern Gigli saw blade. This one was found on our neurosurgery cart.
The pattern differs from the original design.
If anyone has technical insight on the shape of the blade itself, please reply here.
The pattern differs from the original design.
If anyone has technical insight on the shape of the blade itself, please reply here.

Gigli first developed the saw in the 1890's to make an osteotomy in the pelvis in cases of obstructed labor.
He wanted to avoid the pubic symphysis, so he went out a bit and created what was called a 'lateralschnitt' (the blue line below). The pelvis would 'spring open'.
He wanted to avoid the pubic symphysis, so he went out a bit and created what was called a 'lateralschnitt' (the blue line below). The pelvis would 'spring open'.


Gigli's original saw design. It had ebony handles, and the blade could not be sterilized.
From Goodrich 2014, downloadable here:
semanticscholar.org/paper/How-to-g…
From Goodrich 2014, downloadable here:
semanticscholar.org/paper/How-to-g…

Leonardo Gigli was more well known outside of Italy, and much of his work was first published in German.
He was never able to obtain an academic position in Italy, possibly in part due to professional jealously. He died at the age of 44 from pneumonia.
He was never able to obtain an academic position in Italy, possibly in part due to professional jealously. He died at the age of 44 from pneumonia.

Addendum: when in my local hardware store, I looked to see if they had anything like a Gigli saw, and they did have a wire saw for cutting PVC pipe.
The blade is stainless steel and has a different pattern. When asked if the blade could cut femurs, I got no answer. 🧐
The blade is stainless steel and has a different pattern. When asked if the blade could cut femurs, I got no answer. 🧐

• • •
Missing some Tweet in this thread? You can try to
force a refresh